Download
1 / 8
80 likes | 246 Views
Spinal Cord Dysfunction. Neurology Rotation Lecture Series Last Updated by Lindsay Pagano Summer 2013. Case Presentation. The ED consults you on a 15 year old female with LE numbness and weakness. Previously healthy Symptoms began 4 days go with back pain

E N D
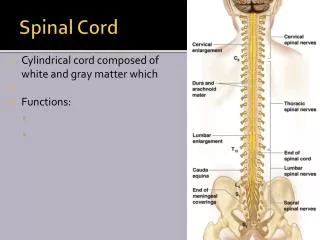
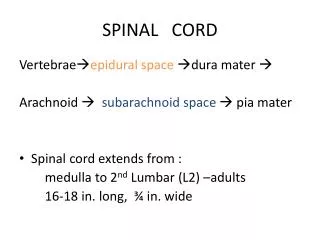
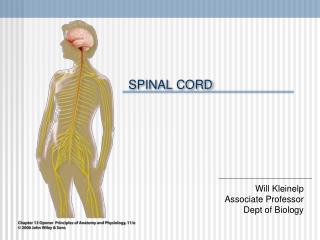
Spinal Cord Dysfunction Neurology Rotation Lecture Series Last Updated by Lindsay Pagano Summer 2013
Case Presentation The ED consults you on a 15 year old female with LE numbness and weakness. • Previously healthy • Symptoms began 4 days go with back pain • Subsequent development of numbness and weakness of both legs • Has lost control of urination and defecation • General exam: + for palpable suprapubic mass • Neuro Exam: normal except for • LE 0/5 throughout and symmetrically with hypotonia • Below the umbilicus, there is complete loss of light touch, temperature and pinprick • BLE with impaired vibration sense • Poor rectal tone • DTRs absent in BLE, toes mute • Differential?
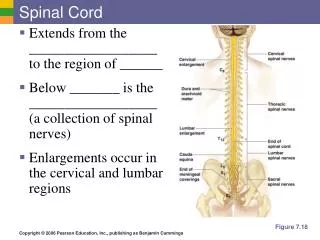
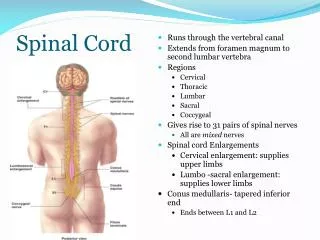
Localizing Spinal Cord Lesions Upper Motor Neuron Lower Motor Neuron aka infranuclear, nuclear; CNS neuron or PNS fibers WEAKNESS flaccid, decreased tone decreased DTRs (efferent limb interrupted) no clonus ATROPHY toes down fasciculations present (exotoxicity) • aka supranuclear, neuron is in CNS • weakness • spastic, increased tone • increased DTRs (muscle spindle threshold decreased) • clonus: contraction of one group mm initiate monotactic reflexes in their antagonists • some atrophy- disuse • toes up • no fasciculations
Localizing the Lesion, continued • History • Onset of symptoms • Incontinence • Sexual dysfunction (depending on age) • Exam • Motor • tone • strength • Reflexes • DTRs • clonus • Sensory • pain and temperature • vibration, joint position sense • sensory level on the trunk • further dermatomes on the extremities
Spinal Cord Lesions • Acutely: Spinal Shock • Initial injury with flaccid paralysis and mute reflexes, including plantar • Gradual recovery and development of UMN, LMN signs • Upgoing toes first to develop • Transverse myelitis: relate to level of lesion; gradual onset; MRI with contrast • MS: related to level of lesion; gradual onset; MRI with contrast • Mass: eg tumor, abscess: related to level of lesion; gradual onset; MRI with contrast • Stroke: typically anterior cord; MRI with diffusion and ADC map • Pain in a band around the abdomen • Symptoms related to level of lesion; sudden onset • Brown-Séquard Syndrome: cord hemisection • IL: weakness, loss of fine touch, vibration, proprioception distal to the lesion • CL: loss of pain and temperature 1-2 levels below the lesion • Atlantoaxial instability: C1-2 articulation • Down syndrome: transverse ligament instability; 10-30% of Down syn patients • Subluxation symptoms are those of cord dysfunction at those levels
PREP question During the health supervision visit for a 6 week old boy, his father expresses concern that his son “doesn’t look like” his other children. Growth parameters are normal except for a head circumference of 35.5 cm (<5th percentile). On PE, you note that the infant does not appear to fixate or track your face visually. There is a “slip through” on vertical suspension and “draping over” on horizontal suspension. DTRs are brisk. Moro reflex is present and brisk. Of the following, the MOST likely cause of this infants hypotonia is: • Anterior horn cell disease • Congenital brain malformation • Congenital myasthenic syndrome • Congenital myopathy • Spinal cord disease
B. Congenital brain malformation • Hypotonia • Localize! UMN versus LMN signs, axial vs appendicular • Take into account growth parameters, especially HC, as well as features such as tracking • Regarding the other choices: A. Anterior horn cell disease: wouldn’t cause microcephaly or increased reflexes C. Congenital myasthenic syndrome: wouldn’t cause microcephaly or brisk reflexes D. Congenital myopathy: no microcephaly or poor visual tracking E. Spinal cord disease: wouldn’t cause microcephaly or poor visual tracking