Download
1 / 1
10 likes | 127 Views
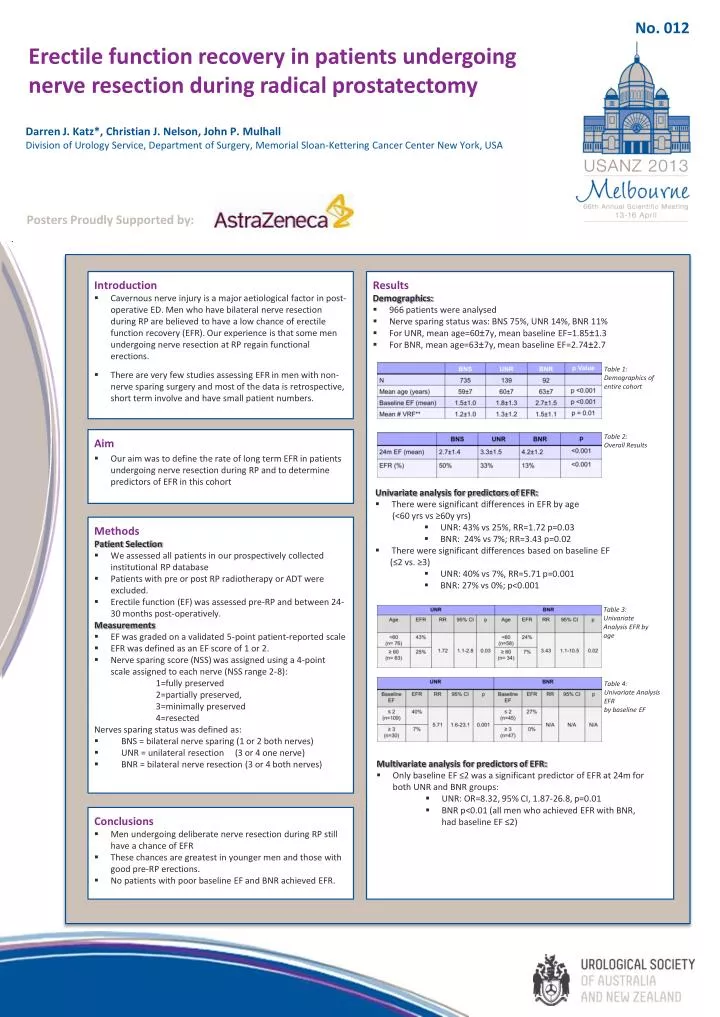
No. 012. Erectile function recovery in patients undergoing nerve resection during radical prostatectomy. Darren J. Katz*, Christian J. Nelson, John P. Mulhall Division of Urology Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center New York , USA.

E N D
No. 012 Erectile function recovery in patients undergoing nerve resection during radical prostatectomy Darren J. Katz*, Christian J. Nelson, John P. Mulhall Division of Urology Service, Department of Surgery, Memorial Sloan-Kettering Cancer CenterNew York, USA Posters Proudly Supported by: • Introduction • Cavernous nerve injury is a major aetiological factor in post-operative ED. Men who have bilateral nerve resection during RP are believed to have a low chance of erectile function recovery (EFR). Our experience is that some men undergoing nerve resection at RP regain functional erections. • There are very few studies assessing EFR in men with non-nerve sparing surgery and most of the data is retrospective, short term involve and have small patient numbers. • Results • Demographics: • 966 patients were analysed • Nerve sparing status was: BNS 75%, UNR 14%, BNR 11% • For UNR, mean age=60±7y, mean baseline EF=1.85±1.3 • For BNR, mean age=63±7y, mean baseline EF=2.74±2.7 Table 1: Demographics of entire cohort Table 2: Overall Results • Aim • Our aim was to define the rate of long term EFR in patients undergoing nerve resection during RP and to determine predictors of EFR in this cohort • Univariate analysis for predictors of EFR: • There were significant differences in EFR by age • (<60 yrsvs ≥60y yrs) • UNR: 43% vs 25%, RR=1.72 p=0.03 • BNR: 24% vs 7%; RR=3.43 p=0.02 • There were significant differences based on baseline EF • (≤2 vs. ≥3) • UNR: 40% vs 7%, RR=5.71 p=0.001 • BNR: 27% vs 0%; p<0.001 • Methods • Patient Selection • We assessed all patients in our prospectively collected institutional RP database • Patients with pre or post RP radiotherapy or ADT were excluded. • Erectile function (EF) was assessed pre-RP and between 24-30 months post-operatively. • Measurements • EF was graded on a validated 5-point patient-reported scale • EFR was defined as an EF score of 1 or 2. • Nerve sparing score (NSS) was assigned using a 4-point scale assigned to each nerve (NSS range 2-8): • 1=fully preserved • 2=partially preserved, • 3=minimally preserved • 4=resected • Nerves sparing status was defined as: • BNS = bilateral nerve sparing (1 or 2 both nerves) • UNR = unilateral resection (3 or 4 one nerve) • BNR = bilateral nerve resection (3 or 4 both nerves) Table 3: Univariate Analysis EFR by age Table 4: Univariate Analysis EFR by baseline EF • Multivariate analysis for predictors of EFR: • Only baseline EF ≤2 was a significant predictor of EFR at 24m for both UNR and BNR groups: • UNR: OR=8.32, 95% CI, 1.87-26.8, p=0.01 • BNR p<0.01 (all men who achieved EFR with BNR, had baseline EF ≤2) • Conclusions • Men undergoing deliberate nerve resection during RP still have a chance of EFR • These chances are greatest in younger men and those with good pre-RP erections. • No patients with poor baseline EF and BNR achieved EFR. • Univariate analysis for predictors of EFR: • There were significant differences in EFR by age (<60 yrsvs ≥60y yrs): • UNR: 43% vs 25%, RR=1.72 p=0.03 • BNR: 24% vs 7%; RR=3.43 p=0.02 • There were significant differences based on baseline EF (≤2 vs. ≥3) • UNR: 40% vs 7%, RR=5.71 p=0.001 • BNR: 27% vs 0%; p<0.001