Download
1 / 20
200 likes | 429 Views
Oncology Pathways. Lung CNG 2009. Intro. Oncology overview Presentation and investigation Oncology Management strategies Stage review Follow up Management of toxicity research. Themes. Early diagnosis Patient selection Pt centred care Investigation and treatment local Expertise

E N D
Oncology Pathways Lung CNG 2009
Intro • Oncology overview • Presentation and investigation • Oncology Management strategies • Stage review • Follow up • Management of toxicity • research
Themes • Early diagnosis • Patient selection • Pt centred care • Investigation and treatment • local • Expertise • Future progress
MCCN Lung Cancer Overview • Presentation and outcomes • Advanced disease • Poor prognosis (23% 1yr survival) • Comparable outcomes cf pt selection (NWCIS 2008) • Devolved care • MDT & pt centred care • Chemotherapy • Satellite radiotherapy • Specialised care • Diagnostic (EBUS) • Pathways: Mesothelioma • radiotherapy • Research • Future Research • Huge potential • Need for greater collaboration
Approach to management Prevention/Screening Early Stage I/II Locally Advanced Stage III Advanced Stage IIIB/IV Surgery ChemoRadiotherapy Chemotherapy radiotherapy concurrent Sequential QOL Cure
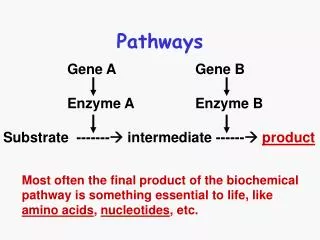
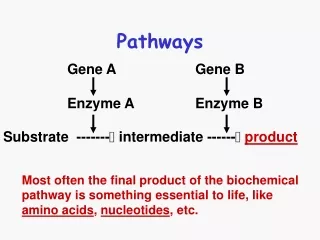
Investigation • PET –CT • Improved staging but • More likely to upstage • False positive rates and treatment delay • Histology • Standard of care for all ? • Move towards individualised management but • May not influence management (poor PS) • May delay treatment decision and palliative care
Histology • Small Cell Carcinoma • AdenoCarcinoma • ERCC1 (DNA repair) • Platinum-resistance • ~50% of samples • EGFR expression • EGFR mutations • Rosell et al, Sept 2009 • 16% of 2100 samples • Predicted by Female, adeno, never-smokers
Rapid Access • Instinctively correct for pt care and reassurance • ? evidence for early diagnosis • CCO SCLC audit 2002-2008 • Outstanding issues • Logistics and clinic design • Patient information and informed consent
Advanced Disease • Stage IIIB and IV bulky LN disease, effusion, distant metastases • Median survival 7-10 mths • Chemotherapy 3-4 cycles standard of care (platinum-doublets) • Important but modest gains in good PS 0-1 patients (NICE Guidance, 2005) • Significant population of borderline cases (PS 2) • Emphasis on patient centred care and QOL • Clinical Trials
Palliative Chemotherapy‘Benefits’ PS 0 No wt loss PS 3 Benefit Toxicity Physical psychological true perceived (pt, doctor, nurse, relative) ?Cost ?Convenience
Recent Advances • Erlotinib (BR21, 2005) • Second/third line general population 2month OS • Maintenance (SATURN): 4weeks OS gain • Bevacizumab (Sandler, 2006) • 2month benefit • Fatal pulmonary haemorrhage • Cetuximab(FLEX Study, 2009) • 4 week benefit in EGFR expressing tumours • Cisplatin-Premetrexed(2009) • Subset analysis in AdenoCa/Large Cell. • 2month survival benefit • Maintenance (JMEN, 2009) benefit • Gefitinib (IPASS Study, 2009) • Benefit in First line EGFR mutations (60% of samples tested) • Selected advanced Adeno, Non-smokers • GefitinibvscarboT • PFS benefit. OS 18.6mths (no difference)
NICE Guidance • First Line • CisplatinPremetrexed (TA181 Sept 09) • Bevacizumab (Withdrawn) • Cetuximab (Ongoing, Rejected EMEA) • Gefitinib 2010 • Erlotinib 2010 • Second line • Erlotinib (TA162 Nov 08) • Alternative to Taxotere in 2nd line
Locally Advanced • Stages IIIA-B • Variable course dependent on T & LN staging • Median survival 14-16mths • Comorbidity issues Progress • Radiotherapy Planning • Hypofractionation, CHART, Stereotactic, IMRT • ChemoRadiotherapy Sequencing • Concurrent 16 vs 13mths
Resection • Adjuvant therapy • Delivery of post op chemotherapy in high risk disease (micro metastases) • T2N1 disease (?large 1B) • Cisplatin-based 2.5-4.1% Absolute benefit • Low numbers (10% resection, PET) • Comorbidity • Trials • MAGRIT (adjuvant vaccination) • 25% NSCLC MAGE 3 expression (poor prognostic feature) • Supportive Phase II data
Follow up • Second Line therapy • Taxotere (7.5 VS 4.6mths) • Erlotinib • Aims/endpoints • Reassurance • Data collection • Identification of recurrence • No impact on survival ? Maintenance trials • No agreed standard FU
toxicities • Pt selection • Toxicity linked to PS and comorbidity • Early mortality 25/15% in Poor PS SCLC/NSCLC • NCEPOD 2008 . • SACT ‘For better, for worse’ • Examples of poor management, pt selection • failings in acute care (35% good) • NCAG & Acute Oncology • Every hospital with A&E should have Acute Oncology Team consisting of Oncology, Nurse Specialists and Admin support • MCCN leading with AOT’s in place 01/04/10
Novel Toxicities& MDT working • Erlotinib • Rash • diarrhoea • Bevacizumab • Bleeding • Hypertension • perforation • Sunitinib • Hand foot syndrome • Arrythmia & QT interval
MCCN Trials Portfolio LLP ?Screening Prevention/Screening Early Stage I/II Locally Advanced Stage III Advanced Stage IIIB/IV ET Trial Fragmatic Lilly Lungstar MAGRIT Surgery ChemoRadiotherapy Chemotherapy SOCCAR NovaRex radiotherapy concurrent Sequential Transitions Breathlessness QUARTZ SCORAD START
Barriers To Research National • Bureaucracy and Research Governance • Eligibility Criteria (PS, comorbidity) Local • Time constraints • Medical Preference (eg QUARTZ) • Patient inconvenience (eg BTOG) • Competition for funds (Industry) • ? Concept of local versus subspecialist care in lung cancer research
conclusions • Majority of patients continue to present with advanced, poor PS and comorbidity • MCCN compares favourably nationally and internationally when comparing Good PS • Emphasis on local delivery of Patient-centred care • Patient selection essential at all points • Need for collaboration and subspecialist care