Download
1 / 27
430 likes | 1.05k Views
Non-Alcoholic fatty liver disease In type 2 Diabetes. Mark Tutschka PGY3 Internal Medicine. Objectives. Understand the epidemiologic significance of NAFLD in T2DM Appreciate the basic pathophysiology of NAFLD and it’s relationship to T2DM

E N D
Non-Alcoholic fatty liver disease In type 2 Diabetes Mark Tutschka PGY3 Internal Medicine
Objectives • Understand the epidemiologic significance of NAFLD in T2DM • Appreciate the basic pathophysiology of NAFLD and it’s relationship to T2DM • Appreciate the clinical features and diagnostic approach to fatty liver disease in diabetic patients • Review the treatment implications of concomitant T2DM and NAFLD
Diabetes – A Growing Problem • 285MM individuals WW; ~3MM Canadians and >20MM U.S. • Among Americans, T2DM accounts for ~17% of all deaths in persons >25 y.o. • The direct healthcare cost of diabetes consumes 2.5-15% of healthcare budgets • WHO predicts WW prevalence of 6.4% by 2030, a 60% increase since 1995 and a 39% rise from 2000 • In 2004-5, 9MM Ontarians were diagnosed with diabetes, a 113% rise over the previous decade ICES Report: The Growing Prevalence of Diabetes in Ontario: Are We Prepared?
Diabetes and NAFLD - Epidemiology • Liver disease is a major contributor to diabetes-related morbidity and mortality • DM is the leading cause of liver disease in Western Countries • Standardized mortality ratio for cirrhosis vs. CVD is 2.57 vs. 1.34 • Cirrhosis is the 4th leading cause of death among diabetics, accounting for ~4-5% of mortality • NAFLD is common • 20-30% of adults in the Western World are estimated to have NAFLD • NAFLD is present in 34-74% of all diabetic patients and in nearly 100% of obese diabetics • Among patients with NAFLD, 50% have NASH and 19% have cirrhosis at the time of diagnosis
NAFLD – What is it? • Defined as fatty liver disease in the absence of EtOH consumption greater than 20g/day • Histologically indistinguishable from alcoholic hepatitis • Encompasses a spectrum or liver pathology • Steatosis - simple fatty infiltration of the liver • NASH / steatohepatitis – steatosis plus inflammation, necrosis and fibrosis • Progresses to cirrhosis in up to 20% of patients
NAFLD / NASH NAFLD NASH
Effects of Insulin Resistance www.cwu.edu/~geed/543/fatty%20acid%20metabolism.ppt Tolman K G et al. Ann Intern Med 2004;141:946-956
NAFLD – Pathophysiology • insulin mediated suppression of lipolysis impaired increased FFA supply to liver • Hyperinsulinemia up-regulates lipogenic transcription factors increased de novo hepaticFFA synthesis • hepatic fat content overwhelms liver’s ability to oxidize excess fatty acid • NAFLD patients increase VLDL-TG secretion, but impaired secretion of apoB100, limiting TG export Lipogenic transcription factors Adams L A et al. CMAJ 2005;172:899-905
NAFLD – Inflammation & Steatohepatitis Dowman J K et al. QJM 2010;103:71-83
NAFLD / NASH – Natural History • Limited prospective follow-up of patients with NAFLD • Patients with NAFLD in the absence of NASH generally follow a benign course • SMR of 1.34 (1.00-1.76) compared to the general population • NAFLD progression to NASH is infrequent relative to progression of alcoholic fatty liver • 3-26% versus 38-50% • NASH progresses slowly, typically over years / decades • 5 and 10 year survival rates of 67% and 59% respectively • 15-20% of NASH patients develop cirrhosis, of these 30-40% incur liver-related mortality
NAFLD – Clinical Features • NAFLD is seen in patients with features of the metabolic syndrome • Obesity: 70-100% have NAFLD • T2DM: 34-75% • Hyperlipidemia: 20-80% • Metabolic syndrome: one-third • Most patients are asymptomatic; signs of chronic liver disease are rare • Liver enzymes fluctuate in NAFLD • Within normal limits at any given time in ~80% of patients • Mild elevations are typical • Ferritin and transferin saturation levels are elevated in >50% of patients • Significance of elevated Fe studies is unclear
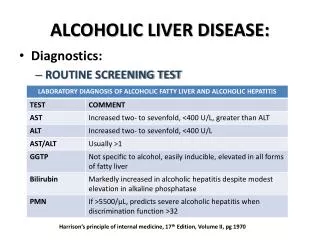
NASH – Clinical Features • Patients who progress to NASH typically remain asymptomatic • Serum AST and ALT are increased in ~90% of patients • AST/ALT ratio is usually <1, a ratio >1 suggests advanced disease • AlkP and Bilirubin are less frequently elevated • Liver enzyme elevation does not correlate with liver histology
NAFLD / NASH - Diagnosis • Suspect NAFLD in any diabetic • Present in >50% of patients • Check liver enzymes in all diabetics • Consider co-existing liver pathology: alcoholic, viral & autoimmune hepatitis, hemachromatosis, Wilson’s disease and α-antitrypsin deficiency • Consider contributing factors, particularly drugs • Glucocorticoids, estrogens, tamoxifen, methotrexate, zidovudine, amiodarone, ASA • Other: TPA, intestinal bypass surgery, rapid weight loss, HIV infection, IBD, bacterial overgrowth, HCV (genotype 3), PCOS, hypothyroidism
NAFLD / NASH - Diagnosis • U/S is useful but has limitations • Sensitivity/specificity – 64%/97% overall, 91%/93% in patients with >30% steatosis • PPV 62-89% • NPV 94% • No utility for NAFLD vs. NASH or for staging • Operator dependent - significant intra- and inter- observer variability • CT has similar diagnostic utility
NAFLD / NASH – Diagnosis, cont’d • A positive U/S in the absence of concomitant liver disease is typically sufficient to diagnose NAFLD • Liver biopsy can distinguish NAFLD from NASH • Severity can also be determined • Liver biopsy is not routinely suggested, consider if: • Uncertainty regarding diagnosis • Manifestations of chronic liver disease • Splenomegaly • Cytopenias • Abnormal iron studies
NAFLD / NASH – Diagnosis, cont’d • Scoring systems have been proposed to determine if fibrosis is present in the setting of NAFLD • BARD • BMI ≥28 – 1 point; AST/ALT ratio ≥0.8 – 2 points; diabetes present – 1point • Score <2 has NPV >90% for advanced fibrosis • AST/ALT ratio (cut-off 0.8) • Sensitivity 74%, specificity 78% NPV 93% for advanced fibrosis • NAFLD Fibrosis Score • Six variables: age, hyperglycaemia, BMI, PLT count, albumin, AST/ALT ratio • NPV 92%, PPV 72% • Online calculator available
Liver Disease & Diabetes – Management Principles • Liver disease does not significantly change the general approach to management of the diabetic patient • Diet and exercise remain a foundation for management • The approach to pharmacologic therapy is essentially unchanged • Hepatic drug metabolism is relatively preserved until patients have evidence of liver failure (ascites, coagulopathy, encephalopathy)
Liver Disease & Diabetes – Management Principles, cont’d • Metformin • Effective first-line therapy in all but the most advanced liver disease patients • At high levels of hepatic impairment ? Increased risk of lactic acidosis • Modest aminotransferase benefits reported in trials of metformin in NASH • TZDs (pioglitazone) • Pioglitazone safe in liver disease despite safety concerns raised by troglitazone • As an insulin sensitizer, a mechanistically rational choice in patients with NASH • Trials in patients with NASH have shown benefit ranging from improved aminotransferases to improved histology • Evidence insufficient to recommend TZDs first-line for NASH, however this is an active research area • Prompt histological recurrence with discontinuation, lack of proven long-term benefit and persistent safety concerns (CHF, liver disease) are barrier to wider use • Not currently recommended in patients with baseline LFTs >2.5x ULN
Liver Disease & Diabetes – Management Principles, cont’d • Sulfonylureas • Generally safe; patients w/significant hepatic impairment may be more prone to lows • Mechanistically not “rational” since they fail to target insulin resistance • Agents with a shorter half-life (glyburide) generally preferred • Meglitinides (repaglinide) • Limited data regarding safety in liver patients • Not associated with hepatic toxicity • Hepatic clearance – titrate up from a low dose • α-glucosidase inhibitors • Mechanistically rationale – “gut specific”, therefore no insulin stimulation and less chance of lows in patients with hepatic dysfunction • RCT of 100 patients demonstrated improved glycemic parameters and decreased ammonia formation • Generally safe in liver patients, however label cautions against use in liver disease because of known mild transaminitis and rarely severe liver disease
Liver Disease & Diabetes – Management Principles, cont’d • Insulin • Reasonable to use in patients with significant hepatic impairment • Factors affecting insulin requirements are significant – monitor patients and adjust doses carefully • Decreased requirement 2o to impaired hepatic gluconeogenesis and decreased hepatic insulin clearance • Increased requirement 2o to insulin resistance
NAFLD/ NASH Principles of Management • Patients with NAFLD generally do not require “treatment” • Biopsy-proven NASH and patients where NASH is suspected (for example by scoring systems) should be considered for more aggressive follow-up • Lifestyle modification (weight loss and exercise) are the main “treatment” • There are no approved pharmacologic treatments for NASH • Guidelines / expert opinion generally do not recommend routine use of any pharmacologic agent
NAFLD/ NASH Management – Lifestyle Modification • A recent systematic review commented on studies evaluating diet, exercise and weight loss for management of NAFLD • Limited data and “considerable heterogeneity” was noted among the various studies identified in the systematic review • Diagnostic criteria /quantitative assessment of NAFLD/NASH • Inclusion and exclusion criteria • Objective monitoring of exercise and use of validated dietary assessment methods • Lack of long-term data • Despite limitations, the authors concluded that lifestyle interventions “producing weight loss significantly improve liver lipid”
NAFLD / NASH Managment – Lifestyle Modification, cont’d • Diet restriction combined with physical activity lowers hepatic enzymes and decreases steatosis when BMI / weight decreases of 7-10% are achieved • Weight loss should be gradual (i.e. 1.5kg/week) - rapid weight loss may accelerate NAFLD NASH • Optimal dietary composition is not well studied • High intake of simple carbohydrates and low intake of polyunsaturated fat is thought to be harmful • Long-term, prospective studies with hard endpoints are lacking
Lifestyle Modification, cont’d • A recent (2010) RCT demonstrated significant improvement by way of lifestyle modification among patients with NASH • 28 patients, randomized 2:1 to intervention vs. placebo (65 patients screened) • Inclusion criteria: elevated AST or ALT, BMI 25-40, no other liver disease • Liver biopsy after 2 week run-in of self monitored diet/exercise • Enrolled based on biopsy proven steatohepatitis • Q12 week fasting blood glucose, liver enzymes. Biopsy after 48weeks • Placebo group attended group session providing basic education regarding NASH, physical activity, diet and weight control • Intervention group: “intensive, state-of-the-art weight loss intervention” based on the Diabetes Prevention Program, LOOK AHEAD” • Target 7-10% weight loss over 6 months and then maintain • Diet: 25% fat; 1000-1200kcal for <200lbs; 1200-1500 for >200lbs • Unsupervised, moderate exercise focusing on walking (goal of 200min/week)
Lifestyle Modification, cont’d • Results • Groups were similar for age, sex, BMI, waist circ., LFTs, lipid profile, HbA1C, metabolic syndrome, anti-glycemic meds • All but one patient completed the study (intervention group) • Weight: -8.7kg vs. -0.5kg (p=.005) • Greater weight loss was achieved by non-diabetics • Liver enzymes: ALT improved significantly (p=.01) in the intervention group; there was no significant difference in AST • On biopsy, overall hepatic steatosis and NASH disease activity decreased significantly in the intervention group (p=.05) • Percent weight loss from baseline correlated significantly with ALT, decreased steatosis and decreased NASH disease activity
Pharmacotherapy • Metformin: • Cochrane Review concluded “improvement in liver enzymes and steatosis without effect on liver histology” • TZDs (pioglitazone): • Improve liver enzymes / steatosis • Conflicting histological results: favourable to no benefit • Discontinuation reverses benefit • Long-term treatment – concern regarding CHF, ? hepatotoxcity • Vitamin E: • Conflicting results ranging from no benefit to improved enzymes and steatosis • Debate continues
Pharmacotherapy • Ursodeoxycholic Acid (UDCA): • Cochrane Review – no significant improvement in LFTs or mortality • Statins: • Generally safe to use in NASH, but no proven hepatic benefit. Recommended only for lipid-related risk factor modification