Download
1 / 30
410 likes | 2.65k Views
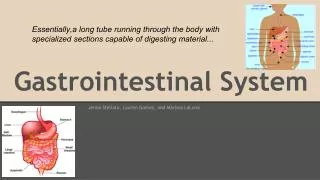
Learning Objectives. Essentials for proper history takingOutline for the health interviewCommon GI sympromsFeatures of abdominal painThe

E N D
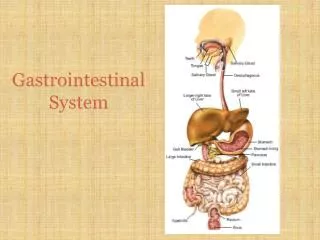
1. History Taking SkillsGastrointestinal System Khaled Jadallah, MD
3. Objectives of History Taking The primary goal of any history taking is to aid the clinician in establishing a diagnosis (or a list of diagnostic possibilities)
It has been estimate that over 70% of diagnoses can be made on history alone
History taking also has other objectives:
It allows the doctor to develop a rapport with their patient,
place the patient�s diagnosis in the context of their life, and
highlight important physical signs that need to be sought on physical examination
4. Outline for the Interview
The Opening
Chief Complaint(s)
History of Present Illness (HPI)
Primary
Secondary (focused ROS): associated symptoms
Tertiary (focused PMH)
Review of Systems
Past Medical History
5. PRESENTING COMPLAINT This may be achieved by asking for e.g. �What problems brought you to the doctors today?�
Use the patient�s own words to describe the chief complaint
The chief complaint and associated symptoms/signs or lab/imaging findings constitute the �clinical problem�
6. The other Pieces of the Puzzle Past medical history
Surgical history
Drug history
Social/occupational history
Family history
7. Common GI Symptoms Globus
Waterbrash/sourbrash
Heartburn
Odynophagia
Dysphagia
Dyspepsia
Nausea
Sitophobia
Vomiting
Anorexia
Retching
Belching
Jaundice
Painful mouth ulcers
Constipation
Obstipation
Diarrhea
Tenesmus
Anal pruritis
Rectal pain/proctalgia fugax
Weight loss
Abdominal pain
Hematemesis
Melena
Hematochezia
Increase in abdominal girth
Bloating/aerophagia
8. Abdominal Pain Third most common complaint of humans
Most common cause of GI consultation
Can be
Hyperacute
Acute
Subacute
Chronic/relapsing
9. Abdominal Pain Visceral Pain - crampy, diffuse, aching
Somatic Pain � localized, intense,
sharp � from irritation of peritoneum
Referred - pain from problem in
another area
Mapping pain may be crucial in initial diagnosis and tests
10. Types of Abdominal Pain Pain from peritoneal irritation � this type of pain is more ominous and is associated with peritonitis of any sort
This pain is generally:
Steady/constant
Often well localized
Not related to peristalsis
Patient often lies still with knees up
11. Referred Pain Abdominal pain is not always confined to the abdomen
Perforated ulcer � can radiate to the shoulder region
Biliary colic � can radiated to the scapula/shoulder region
Renal colic � can radiate to the flank and/or scrotum
Dysmenorrhoea � can radiate to the lower back
12. Features of Abdominal Pain First episode or similar attacks??
Location
Onset
Duration
Frequency
Nature/character
Severity Relation to food ingestion
Aggravating factors
Relieving factors
Radiation
Associated symptoms
Last bowel movement
Effect on function
13. History..What Questions to Ask? Where is your pain? Has it always been there?
Does the pain radiate anywhere?
How did the pain begin (sudden vs. gradual onset)? How long have you had the pain?
What were you doing when the pain began?
What does the pain feel like?
On a scale of 0�10, how severe is the pain?
Does anything make the pain better or worse?
Have you had the pain before?
15. The �Digestive� Pain Digestive tract pain is generally midline
Abdominal pain which is localized to either side suggests that the pain originates from
organs with innervation which is predominantly one-sided (e.g. kidneys, ureters and ovaries), or
structures with somatic innervation
16. Common Conditions Mimicking Acute Abdomen Pneumonia
Angina or MI
Obstructive Uropathy
Hepatitis
Sickle cell crisis
Leukemia
Radiculopathy
Cystitis
Poisons/toxins
Prostatitis
Pyelonephritis
Ureteral obstruction
Vasculitis
Abdominal wall hematoma
Psychogenic
Pericarditis
Herpes Zoster
Acute intermittent porphyria
17. The Acute Abdomen The term �acute abdomen� is usually reserved for a clinical situation in which the patient is suddenly incapacitated by very intense abdominal pain which may or may not be associated with fever, nausea, vomiting or shock
Diagnosis and management depends on information derived both from the history and from the examination.
18. Characteristics of Abdominal Painin Common Surgical Conditions Acute appendicitis
Acute cholecystitis
Perforated ulcer
Small bowel obstruction
Large bowel obstruction
Biliary �colic�
Renal colic
Dissecting/rupture abdominal aneurysm
Rupture ectopic pregnancy
Mesenteric infarction
Abdominal apoplexy (ruptured spleen or liver)
19. Appendicitis Epigastric pain, loss of appetite with or without nausea and vomiting, pain shifting to right lower quadrant
20. Acute Cholecystitis Right upper quadrant or epigastric pain with or without radiation to the back, loss of appetite with or without nausea and vomiting
Previous similar symptoms common, fatty food intolerance common
21. Perforated Ulcer Sudden catastrophic abdominal pain with gradual improvement
Past history of ulcer disease in 50% of cases
22. Small Intestinal Obstruction Cramping abdominal pain, the vomiting of large quantities of fluid, obstipation
Pain subsides after 24 hours of complete obstruction
23. Large Intestinal Obstruction (Carcinoma, Diverticulitis, Volvulus) Similar to small bowel obstruction
Vomiting may be minimal if the ileocecal valve is competent (closed loop obstruction)
24. Biliary �Colic� Sudden onset of acute right upper quadrant or epigastric pain, with nausea, vomiting
The pain is constant�..NOT colicky
25. Renal Calculus Severe abdominal pain, usually unilateral, centering on the flanks and radiating to the groin
Can be associated with nausea and/or vomiting
26. Rupturing Abdominal Aneurysm Sudden onset of severe abdominal, back or flank pain with or without collapse
Often positive history for other atherosclerotic problems
Problem-focused history is a MUST
27. Ruptured Ectopic Pregnancy Complaints suggesting early pregnancy -- missed or abnormal period; diffuse lower abdominal pain
28. Mesenteric Infarction Severe diffuse abdominal pain with or without bloody bowel movement or collapse
Cardiac history frequent
29. Abdominal Apoplexy(Ruptured Spleen, Liver or Blood Vessel) Diffuse abdominal pain, usually without nausea, vomiting. Collapse frequent
History of trauma common
30. Acute vs Chronic Abdominal Pain While acute pain often appears to be more dramatic or serious than chronic pain, one should not assume that chronic pain is any less significant
Patients with gastrointestinal malignancies may present with chronic pain as their primary complaint
Pain which wakes a patient from their sleep or is acute in onset suggests possible strangulation or perforation of the bowel
Pain which is gradual in onset suggests an inflammatory process, such as appendicitis, or an infectious process, such as an abscess
31. Take-Home PointsGeneral Be organized!!
Begin each medical interview with a patient-centered approach
Use open-ended questions initially
Work hard to develop effective doctor-patient communication skills
32. Take-Home PointsGI System GI complaints can be vague and confusing
When confronted with a patient complaining of abdominal pain, the provider must first rule out catastrophic causes of pain
Do not let the location of abdominal pain affect the breadth of your history taking
Remember! GI problems can manifest with extra-GI symptoms, and, extra-GI problems can manifest with GI symptoms
33. On-Line Resources http://www.qub.ac.uk/cskills/video%20resource/GI%20history.htm
http://www.meddean.luc.edu/lumen/meded/MEDICINE/PULMONAR/PD/contents.htm