Download
1 / 19
200 likes | 363 Views
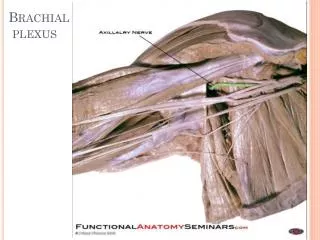
Unusual Case of a Brachial Plexus Disorder. Eddie Patton Jr. M.D, Cecile Phan M.D., Y. Harati M.D. Baylor College of Medicine Neuromuscular Diseases. History.

E N D
Unusual Case of a Brachial Plexus Disorder Eddie Patton Jr. M.D, Cecile Phan M.D., Y. Harati M.D. Baylor College of Medicine Neuromuscular Diseases
History • This is the case of a 44 y/o right handed man who suffered from a sudacuteonset of a slowly progressive right arm weakness and atrophy, particularly of the biceps, beginning 4 months before his presentation to clinic. • Three weeks before presentation he developed right leg pain and weakness • No history of back pain or trauma • No history of bowel or bladder dysfunction
History • PMH: Noncontributory • PSH: Sinus surgery • SH: denies tobacco, ETOH, or illicit drugs, animal groomer who lives at home with his wife • FH: No history of muscle or nerve disorders • ROS: Positive for bi-frontal headaches beginning 2 wks before presentation and decreased sleep
History • Physical exam pertinent positives • Severe atrophy of right biceps • 4/5 strength in right suprascapular, deltoid, brachioradialis, triceps, hand intrinsics, illiopsoas, quadriceps, hamstring, tibialis anterior, extensor hallicus longus • 3/5 strength in right wrist extensors • 1/5 strength in right biceps • Reflexes +1 right brachioradialis and biceps, +3 bilateral patellar and ankle • Babinski absent bilaterally • Sensation mildly decreased to LT and PP right lateral leg
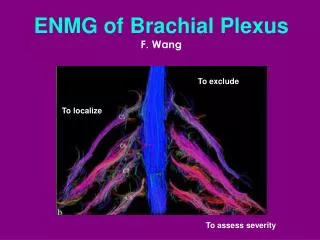
EMG Summary • Neurogenic signs in 3 proximal muscles of the right upper extremity (Biceps C5-6, Infraspinatus C5-6, Triceps C6-8) and one distal muscle (Flexor Carpi Radialis C6-7). • +1 low amplitude reinnervation units in Biceps • Neurogenic signs in 1 distal muscle (Tibialis Anterior) • Comments: “Findings of patchy denervation of the right brachial plexus, predominantly in the C5 and C7 distribution with a non-conductible right musculocutaneous nerve. Mild involvement of the right L4/5 and S1 muscles”
Differential Diagnosis ? • HNPP • Focal variant of CIDP • Vascular (ischemic steal syndrome, thoracic outlet syndrome, subclavian or axillary aneurysm) • Radiation induced plexopathy • Traction or mechanical injury • Neuralgia Amyotrophy ( Parsonage-Turner Syndrome) • Neoplasm • Primary (Schwannoma or nerve sheath tumor) • Secondary ( Pancoast tumor)
Further work-up • MRI brachial plexus
Radiology “Abnormal thickening of the right brachial plexus probably at the level of the superior trunk with enlargement also of the right C5-C6 nerve roots”
Further Work-up? • Focal biopsy of right brachial plexus mass
Semi Thin: onion-bulbs Neuro-filament: axial view of axon staining positive for NF within onion-bulb
Differential Diagnosis ? • Focal nerve enlargement • Schwannoma • Neurofibroma • Solitary circumscribed neuroma • Perineuronoma • Dermal nerve sheath myxoma • Hybrid benign peripheral nerve sheath tumor • Focal CIDP
EMA and S-100 protein stains • “ EMA confirms the formation of concentric rings of positively staining spindle cells consistent with perineurial cells. Although S100 is positive in axons, it is a dominant component of nonlesional nerve” • “Subsequent review of electron microscopy shows both Schwann cells and cells with discontinuous basal lamina and occasional pinocytosis surrounding centrally placed axons”
Perineurioma • 1978- Lazarus and Trombetta coined term after case of a 45 y/o man with a calf tumor • Clinically presents as progressive loss of motor function • Sensory deficit and pain are uncommon • True tumor consists of whorls and fascicles of spindle cells with ultrastructure of perineurial cells • Incomplete basal lamina • Poorly formed tight junctions • Pinocytotic vesicles • Gold Standard- + EMA stain and – S-100 • Neoplastic perineurial cells express immunoreactive epithelial membrane antigen (EMA) • Schwann cells immunoreactive to S-100 protein
Treatment of Nerve Sheath Tumors Observation Surgical removal Controversial