Download
1 / 17
300 likes | 2.1k Views
Gingival Curettage. Wilkins, chapter. Learning Objectives. Distinguish between gingival and subgingival curettage Identify the indications & contraindications for gingival curettage Describe the procedure Describe the healing that takes place following curettage. Introduction.

E N D
Gingival Curettage Wilkins, chapter
Learning Objectives • Distinguish between gingival and subgingival curettage • Identify the indications & contraindications for gingival curettage • Describe the procedure • Describe the healing that takes place following curettage
Introduction • Refers to the scraping of the pocket wall • Separates diseased soft tissue • Inadvertent curettage occurs with periodontal debridement
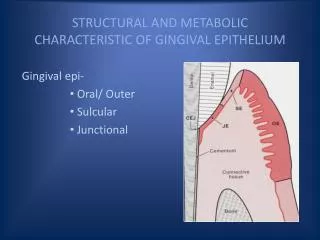
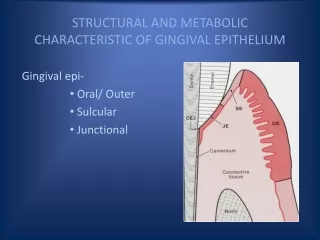
Definitions • Gingival Curettage: • Removal of inflamed soft tissue • Removes diseased sulcular & junctional epithelium • Indications: pseudopockets, shallow true pockets • Objective: gingival shrinkage
Definitions • Subgingival Curettage: • Performed apical to epithelial attachment • Removes connective tissue attachment down to alveolar crest • Indications: deep pockets • Objectives: reattachment
Rationale • Removes granulation tissue • Within granulation tissue we find: • Areas of chronic inflammation • Bacteria, calculus • Epithelial tissue lines granulation tissue • May pose barrier to new fiber attachment
Rationale • However, • Granulation tissue slowly resorbs following debridement • Bacteria eliminated • Tissue heals • Questionable: • Whether curettage significantly improves health of tissue beyond what is seen with periodontal debridement
Indications • Generally limited: • Moderately deep infrabony pockets where new attachment attempted • Closed surgery advised • Technically difficult procedure • Inadequate accessibility • When surgical techniques not advised • Due to age, systemic problems • Goal of pocket elimination compromised
Indications • Maintenance therapy • In areas of chronic inflammation, especially if client has had pocket reduction surgery
Basic Technique • Periodontal debridement performed prior to curettage • Tissues anaesthesized • Appropriate selection of instruments • Curettes, universal curette • Curette blade placed against tissue • Horizontal stroke
Basic Technique • Irrigate tissues to flush out debris • Gentle finger pressure applied to adapt tissues • Separated interdental papillae may require sutures • Surgical dressing may be indicated
Other Techniques • Excisional New Attachment Procedure • Ultrasonic Curettage • Chemical Curettage • Laser Fiber Curettage • Students can do their own research on the above techniques
Healing Following Debridement & Curettage • Uneventful healing • Formation of long junctional epithelium • No significant differences when compared to debridement therapy alone
Curettage using Laser Fiber Fiber tip slowly inserted into pocket & kept parallel to tooth Usually painless Moved apically until pocket base reached Vaporizing of pocket epithelium, subgingival plaque & some granulation tissue occurs
Curettage using Laser Fiber Fiber, held in contact with root surface, is slowly moved coronally & withdrawn This vaporizes microbial debris on root surface Any remaining deposits can be removed with a curette
Results of Curettage - Laser Fiber Before treatment – pockets measure 7-8 mm
Results of Curettage - Laser Fiber Just after treatment 3 months after treatment – 3 mm pockets