Download
1 / 34
340 likes | 692 Views
www.brainage.med.unsw.edu.au. THE BRAIN AND AGEING PROGRAM. University of New South Wales Southeastern Sydney Illawara Area Health Service Neuropsychiatric Institute Department of Old Age Psychiatry Prince of Wales Hospital. BRAIN AND AGEING PROGRAM. Primary aims

E N D
www.brainage.med.unsw.edu.au THE BRAIN AND AGEING PROGRAM University of New South Wales Southeastern Sydney Illawara Area Health Service Neuropsychiatric Institute Department of Old Age Psychiatry Prince of Wales Hospital
BRAIN AND AGEING PROGRAM Primary aims • To conduct research into ageing and disorders of the brain, particularly neuropsychiatric disorders of older people and disorders of cognition, including the dementias. • To develop the highest standards in the clinical practice of the neuropsychiatry and neuropsychology of ageing. • To promote education and dissemination of information about brain disorders and ageing. • To contribute to the development of social policy in relation to older citizens with brain disorders.
Now Then
THE AGEING BRAIN • Brain changes with age: • Atrophy of gyri • Widened sulci • Enlarged ventricular system • Brain weight shrinks: • 5% by 70 years • 10% by 80 years • 20% by 90 years P.Sachdev@unsw.edu.au
COGNITIVE CHANGES WITH AGEING • Great heterogeneity • Reaction time is increased and speed of information processing reduced • Medium-term memory decreases with age • Working memory, semantic memory and linguistic abilities remain stable • Confounding effects of dementia, depression, sensory deficits and physical illness • Cohort or generation effects • Education and premorbid IQ are important considerations P.Sachdev@unsw.edu.au
NEUROLOGICAL SIGNS WITH AGE • Loss of upward gaze • Essential tremor • Increased tone, especially of lower limbs • Loss of vibration sense predominantly in lower limbs • Orofacialdyskinesias • Gait abnormalities: postural flexion, reduced arm swing, reduced balance P.Sachdev@unsw.edu.au
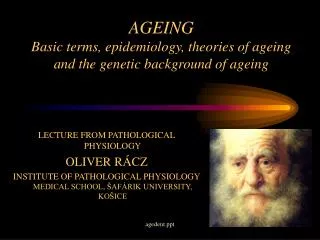
Madame Jeanne Calment of Arles, France, photographed in 1994 at the age of 119. She died in 1997, aged 122, of ‘natural causes’. “Living independently until the age of 110….. Despite visual and hearing loss, she maintained autonomy in the face of the dependence imposed by the regulations of a nursing home - refusing care and visitors she did not want, smoking in a public place, and insisting on her daily glass of port..” Ritchie, 1997 P.Sachdev@unsw.edu.au
NEUROPATHOLOGY OF ALZHEIMER’S DISEASE NEURITIC PLAQUE (central amyloid core) NEUROFIBRILLARY TANGLE (paired helical filaments) Silver stain P.Sachdev@unsw.edu.au
Deep white matter hyperintensities Focal Focal confluent P.Sachdev@unsw.edu.au Diffusely confluent Extensive
BRAIN AND AGEING PROGRAM • Sydney Stroke Study (SSS) (1997-) • Memory and Ageing Study (MAS) (2005-) • Older Australian Twins Study (OATS) (2006-) • PATH Through Life Study (1998-) • Sydney Centenarian Study (2007-) • Falls and balance in ageing and dementia (2005-) • Nursing Home Study • Dementia in General Practice • Neuropathology of brain reserve • Stem cells for dementia • Genetics of dementia • Brain imaging
Healthy Controls Admission to hospital N=1050 N = 130 Meets entry criteria Baseline assessment SYDNEY STROKE STUDY N=252 3-month assessment N=103 (N=96) Medical Neuropsychological Psychiatric MRI (Structural) 1H-MRS MR perfusion N=210 (176 + 34) 15-month assessment N=86 N= 142 3 year FU N=74 N= 88 N=68 5 year FU N=64
Our study supports the contention that stroke leads to subtle changes in cognitive functioning in many patients. Immediately after a stroke, patients are usually concerned about its impact on physical functioning, and it is only later that mental functioning comes into focus. Cognitive impairment is common in stroke patients. More than 50% had some level of cognitive impairment, which was severe in about 25%. Those with larger strokes and who started with a lower baseline function were more likely to have cognitive problems • Sachdev PS, Brodaty H, Valenzuela MJ, Lorentz L, Looi JCL, Wen W, Zagami A. The neuropsychological profile of vascular cognitive impairment in stroke and TIA patients. Neurology 2004;62:912-919. • Sachdev PS, Brodaty H, Valenzuela MJ, Lorentz L, Koschera A. Progression of cognitive impairment in stroke patients. Neurology 2004;63;1618-1623. • Sachdev PS, Brodaty H, Valenzuela MJ, Lorentz L, Looi JCL, Berman K, Ross A, Wen W, Zagami A. Clinical determinants of dementia and mild cognitive impairment following ischaemic stroke: the Sydney Stroke Study. Dementia & Geriatric Cognitive Disorders 2006; 21:275-283.
The cognitive deficits seen in stroke patients and those with Vascular Dementia are qualitatively different from those seen in Alzheimer’s Disease. Sachdev PS, Brodaty H, Valenzuela MJ, Lorentz L, Looi JCL, Wen W, Zagami A. The neuropsychological profile of vascular cognitive impairment in stroke and TIA patients. Neurology 2004;62:912-919.
Stroke patients show changes in their brain scans that pre-date the stroke, suggesting that cerebrovascular disease may affect the brain in more ways than simply through strokes. It also suggests that preventative efforts should begin much earlier, predating the stroke by many years. • Wen W, Sachdev P. The topography of white matter hyperintensities on brain MRI in middle-aged individuals. NeuroImage 2004; 22(1):144-154. • Wen W, Sachdev PS. The extent and distribution of white matter hyperintensities in stroke patients: the Sydney Stroke Study. Stroke 2004; 35:2813-2819.
Homocysteine has emerged as another risk factor to watch in those who are prone to strokes. Sachdev P. Homocysteine, cerebrovascular disease and brain atrophy. [Proceedings of the First Congress of the International Society for Vascular Behavioural and Cognitive Disorders (VAS-COG 2003)] Journal of Neurological Sciences 2004; 226:25-29.
White matter hyperintensities on MRI scans are common in healthy individuals and may represent regions of reduced blood supply. They tend to increase by about 10% per year, and may cause impairment in cognitive and motor function. Sachdev P, Wen W, Chen X, Brodaty H.Progression of white matter hyperintensities in elderly individuals over 3 years. Neurology 2007; 68:214-222. .
Proton spectroscopy is a useful technique to monitor changes related to ageing, and can be used to predict who will develop cognitive decline following stroke. It complements other forms of brain imaging and may have clinical application for this purpose. Ross AJ, Sachdev PS, Wen W, Brodaty H. Longitudinal Changes During Aging Using Proton Magnetic Resonance Spectroscopy, Journal of Gerontology: MEDICAL SCIENCES, 2006;61A(3)291-298 Ross AJ, Sachdev PS, Wen W, Brodaty H. Prediction of cognitive decline after stroke using proton magnetic resonance spectroscopy, Journal of Neurological Sciences, 2006; 251:62-69
Sachdev PS, Chen X, Joscelyne A, Wen W, Brodaty H. The amygdala in stroke/TIA patients and its relationship to cognitive impairment and psychopathology: The Sydney Stroke Study. American Journal of Geriatric Psychiatry 2007; 15:487-496. • Sachdev PS, Chen X, Joscelyne A, Wen W, Altendorf A, Brodaty H. Hippocampal size and dementia in stroke patients: The Sydney Stroke Study. Journal of the Neurological Sciences 2007. The hippocampus and amygdala are affected early in Alzheimer’s disease, but the pathology of stroke or vascular dementia does not necessarily affect it specifically. In these papers, we show that patients with stroke have smaller hippocampi and amygdalae, which relate to their cognitive status. It is uncertain whether this is due to associated Alzheimer pathology, or due to abnormalities of blood supply. The study suggests that a small hippocampus may not help distinguish Alzheimer’s disease from vascular dementia.
In the first year after the stroke, over a third of patients had significant levels of apathy. This needs to be distinguished carefully from depression as its treatment is quite different. Brodaty H,SachdevP, Withall A, Koschera A, Valenzuela M, Lorentz L. Frequency and clinical, neuropsychological and neuroimaging correlates of apathy following stroke-The Sydney Stroke Study, Psychological Medicine, 2005;35:1707-1716.
http://train.headstrongcognitive.com/ Valenzuela M, Sachdev P. Assessment of complex mental activity across the lifespan: development of the Lifetime of Experiences Questionnaire (LEQ). Psychological Medicine 2007; 37:1015-1025. • Lifetime of Experiences Questionnaire (LEQ): • This is a new scale developed to measure mental activity through the life span as an indicator of brain reserve
Brodaty H, Altendorf A, Withall A, Sachdev PS. Doing well after stroke – The Sydney Stroke Study (in submission). Fifteen months after their stroke, about a third of patients were doing well in their cognitively and functionally (ie abilities in thinking and managing day-to-day tasks), a third were doing poorly on both and a third had mixed outcome. As expected younger patients were doing better as were those who had less brain atrophy (ie shrinkage) and did not have atrial fibrillation (a specific abnormal rhythm of the heart).
We found that about one in four patients had significant depression in the 15 months after a stroke, with the rate increasing from month 3 to month 15. The majority of cases were not receiving any treatment for this, implying a need for greater awareness among doctors, patients and their families. Brodaty H, Withall A, Altendorf A, Sachdev P. Rates of depression at 3 and 15 months Poststroke and their relationship with cognitive decline: the Sydney Stroke Study. American Journal of Geriatric Psychiatry 2007; 15:477-486.
www.brainage.med.unsw.edu.au • Contact • Lauren NortonAdministrative AssistantBrain and Ageing ProgramSchool of Psychiatry, The University of New South WalesNeuropsychiatric Institute, Euroa Centre, Prince of Wales HospitalRandwick NSW 2031AustraliaT +61 (2) 9382 2094F +61 (2) 9382 3774E l.norton@unsw.edu.au
Psychiatrists P Sachdev, H Brodaty, J Looi, B McIvor, J Bakas Neurologists D Gillies, A Zagami, M Hersch, D Pryor, R Johnston, J Enis Neuroradiologist R Shnier Neuroimaging W Wen, A Ross Research Psychologists M Valenzuela, L Lorentz, J Kinch, M Jones, A Walker, J Sims, A Koschera, A Withall Research clinicians D Monk, L Howard, A Woods Genticist X L Wang, S Easteal Adm assistants E Milne, P Sawdy, W Schinke SYDNEY STROKE STUDY TEAM Financial support of the National Health & Medical Research Council, Univ New South Wales, Rebecca Cooper Foundation, Fairfax Foundation and Old Age Psychiatry Trust Fund