Download
1 / 50
570 likes | 1.34k Views
Anatomy & Biomechanics of the Shoulder. James J. Irrgang, Ph.D., PT, ATC Department of Physical Therapy University of Pittsburgh. Shoulder Motion. Combined Movements:. Flexion - 150 - 180 0 Extension - 50 - 60 0 Abduction - 150 - 180 0 External rotation - 90 0

E N D
Anatomy & Biomechanics of the Shoulder James J. Irrgang, Ph.D., PT, ATC Department of Physical Therapy University of Pittsburgh
Shoulder Motion Combined Movements: • Flexion - 150 - 1800 • Extension - 50 - 600 • Abduction - 150 - 1800 • External rotation - 900 • Internal rotation - 70 - 900 • Horizontal abduction • Horizontal adduction
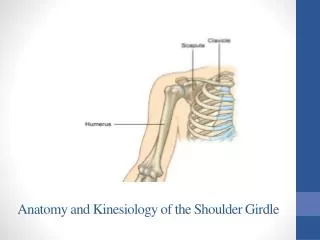
Shoulder Girdle Includes: • G-H joint • A-C joint • S-C joint • S-T joint • Subacromial space
Glenohumeral Motion Controlled by: • Passive restraints • Active restraints
Glenohumeral Motion Passive Restraints: • Bony geometry • Labrum • Capsuloligamentous structures • Negative intra-articular pressure
Capsuloligamentous Structures Glenohumeral ligaments: • SGHL • MGHL • IGHL complex • anterior band • posterior band • axillary pouch
Capsuloligamentous Structures Glenohumeral ligaments:
Capsuloligamentous Structures • Coracohumeral ligament • anterior band • posterior band
Restraints to External Rotation Dependent on arm position: • 00 - SGHL, C-H & subscapularis • 450 - SGHL & MGHL • 900 - anterior band IGHLC
Restraints to Internal Rotation Dependent on arm position: • 00 - posterior band IGHLC • 450 - anterior & posterior band IGHLC • 900 - anterior & posterior band IGHLC
Restraints to Inferior Translation Dependent on arm position: • 00 - SGHL & C-H • 900 - IGHLC
Glenohumeral Motion Scapular Plane: • Flexion/extension - 1200 • Abduction/adduction - 1200 • External/internal rotation • Horizontal abduction/ adduction
Glenohumeral Motion Convex - Concave Rule:
Glenohumeral Motion Arthrokinematics: • Abduction • Flexion • Extension • External rotation • Internal rotation
Glenohumeral Motion Arthrokinematics: Harryman et. al. 1990
Glenohumeral Motion Arthrokinematics: Harryman et. al. 1990
Glenohumeral Motion Arthrokinematics: Harryman et. al. 1990
Glenohumeral Motion Capsular Tightness: Results in Abnormal Arthrokinematics
Glenohumeral Motion Normal Arthrokinematics: Combines rotation & translation to keep humeral head centered on glenoid
Deltoid Pectoralis major Latissimus dorsi Teres major Biceps Coracobrachialis Triceps Scapulohumeral Muscles Prime Movers:
Scapulohumeral Muscles Rotator Cuff: • Subscapularis • Supraspinatus • Infraspinatus • Teres Minor
Rotator Cuff Function • Approximates humerus to function • Supraspinatus assists deltoid in abduction • Subscapularis, infraspinatus & teres minor depress humeral head
Subscapularis • Effective restraint to ER with arm at side • Ineffective restraint to ER with arm abducted to 900 Turkel et. al. JBJS 1981
Infraspinatus/Teres Minor • Reduces strain on anterior band of IGHLC • “Hamstrings” of glenohumeral joint Cain et. al. AJSM 1987
Long Head of Biceps • Biceps tendon force increases torsional rigidity to ER • No effect on strain of IGHLC • Effect lost with SLAP lesion Rodosky et. al. AJSM 1994
Biceps Becomes More Important Anterior Stabilizer as Capsuloligamentous Stability Decreases Itoi et. al. JBJS 1994 & Glousman et. al. 1988
Force Couples Acting on Glenohumeral Joint • Transverse plane - anterior vs. posterior RC • Coronal plane - deltoid vs. inferior RC
Rotator Cuff Tear Supraspinatus: • Essential force couples maintained • Normal strength & function possible
Rotator Cuff Tear Supraspinatus/Posterior Cuff: • Essential force couples disrupted • Weakness with external rotation • Little active elevation possible
Rotator Cuff Tear Massive Tear : • Essential force couples disrupted • Weakness with internal & external rotation • Little active elevation possible
Structures Within Suprahumeral Space • Long head of biceps • Superior capsule • Supraspinatus tendon • Upper margins of subscapularis & infraspinatus tendons • Subacromial bursa • Inferior surface of A-C joint
Subacromial Space Clinical Relevance: • Avoidance of impingement during elevation of arm requires: • external rotation of humerus to clear greater tuberosity • upward rotation of scapula to elevate lateral end of acromion
Subacromial Space Clinical Relevance: • Primary impingement: • structural stenosis of subacromial space • Secondary impingement: • functional stenosis of subacromial space due to abnormal arthrokinematics
Scapulothoracic Muscles • Trapezius • Serratus anterior • Rhomboids • Levator scapulae • Pectoralis minor • Subclavius
Scapulothoracic Motion • Elevation/depression • Protraction/retraction • Upward/downward rotation
Force Couple atScapulothoracic Joint • Serratus anterior produces anterio-lateral movement of inferior angle • Upper trapezius pulls scapula medially
Scapulohumeral Rhythm • Total elevation: • 1200 at G-H joint • 600 at S-T joint
Force Couple atScapulothoracic Joint • Serratus anterior produces anterio-lateral movement of inferior angle • Upper trapezius pulls scapula medially
Acromioclavicular Joint • Joint capsule • A-C ligaments • Intra-articular disc • Coracoclavicular ligaments • conoid (medial) • trapezoid (lateral)
Acromioclavicular Joint Movements: • Axial rotation of clavicle (spin) • Angulation between scapula & clavicle
Sternoclavicular Joint • Joint capsule • Anterior & posterior S-C ligaments • Intra-articular disc • Interclavicular ligament • Costoclavicular ligament
Sternoclavicular Joint Motions: • Protraction/retraction • Elevation/depression • Axial rotation (spin)
Biomechanics of Scapular Rotation • Scapulothoracic motion occurs as part of closed kinetic chain involving: • A-C joint • S-C joint
Scapular Rotation Phase I • Upper & lower portions of trapezius & serratus anterior produce upward rotatory force on scapula • Motion at A-C joint prevented by coracoclavicular ligament • Rotation of scapula occurs as elevation of clavicle at S-C joint
Scapular Rotation Phase II • Further motion at S-C joint prevented by costoclavicular ligament • Continued upward rotation of scapula pulls on costoclavicular ligament causing posterior rotation of clavicle • Posterior rotation of clavicle allows further upward rotation of scapula
Scapular Rotation Necessary to: • Enhance glenohumeral stability • Elevate acromion to avoid impingement • Maintain effective length tension relationship of scapulohumeral muscles Review this lecture