Download
1 / 29
320 likes | 988 Views
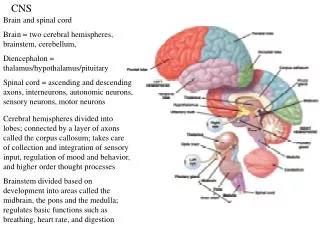
CNS tumors. Dr. Waleed Dabbas. Background. Frequency. Children : -Posterior fossa tumors ( Infra-Tentorial). - Astrocytoma, Ependymoma, and Medulloblastoma. Adults : -The most common malignant brain tumor in adults is GBM. Incidence.

E N D
CNS tumors Dr. WaleedDabbas
Frequency Children : -Posterior fossa tumors ( Infra-Tentorial). -Astrocytoma, Ependymoma, and Medulloblastoma. Adults : -The most common malignant brain tumor in adults is GBM.
Incidence • Overall incidence of primary brain tumor is 9.5 cases per 100,000 population in the United States. • More than 50% are gliomas • Brain tumors represent 30% of all childhood malignancies
Epidemiology • Gender • Slight increased brain tumors in males • Two peaks • Smaller peak in pediatric age group • Second peak in elderly population between 70-80 years of age
Etiology and Risk Factors • Several genetic disorders cause or increase risk for brain tumors. • Neurofibromatosis • Tuberous sclerosis • Turcots syndrome • Osler-Weber-Rendu syndrome • Li-Fraumeni syndrome
Symptoms and signs • Seizures – 54% at presentation • Headaches – 71% • Mental change – 53% • Hemiparesis – 43% • Cranial nerve – 14%
Brain tumor syndromes • Seizure : Cortical lesion • Behavioral : Anterior Cranial fossa. • Weakness: internal capsule or primary motor cortex • Vision : optic nerve compression • Speech: Broca’s area. • Endocrine : prolactinoma , etc.. • Torticollis : post. Cranial fossa tumor compressing the XI nerve. • Anosmia : Foster-Kennedy Syndrome ( ant. Cranial fossa tumor ) “ ipsilateral Optic nerve atrophy + Contralateralpapilledema “
Diagnosis • Imaging studies available are MRI • On MRI the high grade of malignant gliomas appear as contrast enhancing mass lesions • CT scan • Contrast enhanced CT scan for use if MRI is unavailable • Nuclear medicine studies • Brain scan not used much now
Classifications By origin : Primary VS secondary By location : supratentorial VS infratentorial By cell type e.g. glioma,menengioma,oligodendroglioma>>> By grade: 1,2,3,4 Benign VS malignant ?
Menengiomas • Benign, Rarely malignanat • Can grow at any part of the meninges, common sites: cerebral convexity, falx cerebri, parasagital. • Age: 40-50 . • More in Female “ progesterone receptors on meningiothelial cells” .
Hemangioblastoma • Benign • Most common adult Primary Post. Cranial Fossa tumor • Highly Vascularized • Two forms : Cystic VS. Solid.
Neuroepithelial TumorsGLIOMA Type of Cells: A. Astrocytic tumors B. Oligodendroglial tumors C. Ependymal tumors D. Mixed gliomas E. Choroid plexus tumors Grade: Low VS. High Location: SupraTentorial VS. InfraTent.
Astrocytoma Grade I & II:- Superficial & Infratentorial. ( Benign ) - Young ages(Juv. Cerebellar Astrocytoma) Grade III & IV: Anaplastic Astrocytoma Glioblastoma Multiforme
Oligodendroglioma • Microcalcification is common. • Well differentiated VS Anaplastic “less common”
Ependymoma • Ependymal cells that line the ventricles. • less than 2% of brain tumors. • Usually low grade histology but have a high grade of recurrence • Supratentorial 3rdventricle+malignant Infratentorial 4thventricle+Benign“more common”
Choroid Plexus Papilloma* Rare * • From the Choroid plexus inc.CSF production Hydrocephalus. • Supratentorial Children ( Lateral Vent. ) Infratentorial Adult ( Rare )
Medulloblastoma • PNET (30% of pediatric brain tumors ) • Midline in the vermis of the cerebellum & extend to the 4th ventricle. • Young, hydroceph., ataxia. • Spread through CNS, bone.
Pituitary tumors Pituitary tumors have three features: Local mass effect Visual field disturbance (bitemporal hemianopia). headache Hormone deficiency: deficiency tend to first suppress LH and GH, followed in sequence by loss of TSH,ACTH and FSH Hormone excess
Craniopharyngioma Derived from remnants of the structures that give rise to pituitary gland. Mass effect (headache, visual field defect) Hormonal deficiencies Could be cystic or solid with or without calcification.
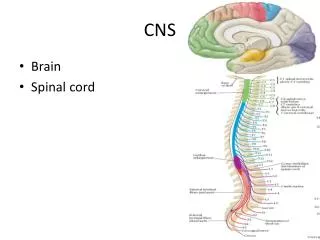
Spinal tumors 1 Extradural : Secondary deposits in the spine(commonest) primary vertebral bony tumors(osteoclastoma,myeloma) Lymphomas 2 Intradural extramedullary Meningioma Neurofibroma 3 Intramedullary (rare) Glioma Ependymoma Others such as hemangioma
Involvement of the CNS by Systemic Cancer • Brain metastases occur in 25-35% of all cancers. • The peak incidence of brain metastases is bimodal ages 0-10 years and age 55-59 years. • Location • 50% of brain metastases are supratentorial • Lung cancer and breast cancers are most common metastatic tumors to the head. • Melanoma has greatest potential for metastasis to the brain. • Approximately 40% of all patients with systemic disease develop brain metastases.
Prognostic Factors • Include pathological grade, patient age and overall patient function at the time of diagnosis and duration of symptoms. • Immediate survival with resection, radiotherapy and chemotherapy is three years for those with anaplastic astrocytoma and one year for those with glioblastoma multiform.
Treatment • Includes supportive and definitive treatment • Supportive agents are anticonvulsant and corticosteroids • Definitive therapy for intracranial tumor is surgery
Treatment • Surgical tools available include: • Stereotactic frames • Definition provided three dimensional imaging system for accurate targeting of brain lesions identifed on CT or MRI scan • Image based guiding system • Definition frameless for image guided stereotactic system. Use computer technology to co-register pre-operative imaging studies with intra-operative head position. These systems facilitate more complete tumor resection.
Radiation Therapy • Radiation plays a central role in treatment of brain tumors in adults. • Whole brain versus partial brain radiation • Dose to the response of low grade gliomas • Other alternatives to conventional radiotherapy include hyperfractionated radiotherapy or use of radiosensitizers and boron neutron capture therapy
Chemotherapy • Chemotherapy regimens for gliomas include: • Single agent BCN4 or combination chemotherapy of CCNU, procarbazine and vincristine