Download
1 / 18
180 likes | 381 Views
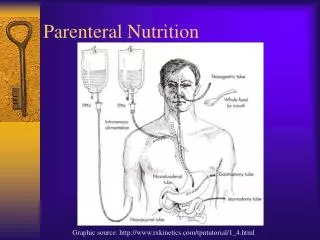
A mixed bag: an enquiry into the care of hospital patients receiving parenteral nutrition. Neena Modi Vice President, Science & Research Royal College of Paediatrics & Child Health Professor of Neonatal Medicine Imperial College London . Disclosures.

E N D
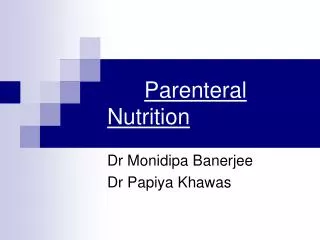
A mixed bag: an enquiry into the care of hospital patients receiving parenteral nutrition Neena Modi Vice President, Science & Research Royal College of Paediatrics & Child Health Professor of Neonatal Medicine Imperial College London
Disclosures • Views of Expert Group members and advisors sought • Neonatal clinician in a tertiary centre • Lead a research programme involving newborn nutrition • Advised the Chief Pharmacist’s survey of neonatal PN in 2008/9
What we knew • Essential is the smallest, sickest babies • The target is growth, not correction of malnutrition • Standard regimens feasible • Often Partial (not Total) PN, bridging the gap to full milk feeds • Documentation poor and variable • Prescribing and dispensing processes variable • Complications common • Babies are neither small children nor adults • Some 1,500 to 3,000 babies receive PN in the UK each year
Confidential enquiries “The purpose of a confidential enquiry is to detect areas of deficiency in clinical practice and devise recommendations to resolve them; enquiries can also make suggestions for future research programmes”
24% 12 babies
Key findings • “Good practice”, defined as a “standard that you would accept from yourself, your trainees and your institution”, identified in 24% (62/264) of neonatal cases • Delay in recognising need for PN in 28% • Delay in starting PN once decision made in 17% • Poor documentation in 72% • First PN provided considered inadequate in 37% • Metabolic monitoring inadequate in 19%
Principal recommendations • Prompt consideration of need for PN, start without delay • First PN must be appropriate to neonate’s needs • Close monitoring essential • Neonatal units should have policies for documentation • Team approach • Consensus on best PN practice • Education, audit and training needed • NICE guidelines for nutritional support needed • Central hospital record of patients receiving PN • Attention to vascular line care
What was missing? • Details of prescribing and dispensing practice (Chief Pharmacist’s 2009 Study) • Denominators (how many babies should have received PN?) • Controls (were complications reliably attributable to PN?) • Details of concurrent milk feeds (was nutritional support really poor?) • A sense of what variation in practice there was among assessors (was the enquiry consistent?) • Acknowledgement that the evidence base is poor
Possible questions • Are process or outcome measures the best means for neonatal services to evaluate their practice? • What specific measures should be audited? • Is adequacy of PN the right question? • Which processes (prescribing, preparing, dispensing, delivering) require standardisation? • What is the research gap?
Optimal growth targets are not known Preterm nutrition is • Controversial • Variable • Poorly evidenced • Focused on growth outcomes even though the optimal pattern of growth is unknown
Optimal nutrient requirements for preterm babies are not known • Intrauterine nutrient provision • lipid - minimal • glucose - moderate • amino acid - high • Postnatal nutrient provision • lipid - high • glucose - high • protein - low
Other dangers Parenteral nutrition, (whether administered centrally or peripherally) (IRR 13.8, 95% CI 8.5 to 22.3, p<0.001) and gestational age < 26 weeks (IRR 2.4, 95% CI 1.7 to 3.5, p<0.001) are the highest significant independent risk factors for newborn late onset blood stream infection (Modi et al 2006)
The tightrope of preterm nutrition support • Not too much, not too little, but just right • NEON (Nutritional Evaluation and Optimisation in Neonates trial) commenced recruitment June 2010
Our conclusions • The call to improve practice is welcomed • The focus on the newborn and on children is applauded • The need for consistency of prescribing, dispensing, delivering and documenting is strongly supported • Preterm nutrition is experimental, research is needed • Beware the implementation of nutritional guidance that lacks an evidence base
Food for thought • Target methodology to specific patient group • Denominator capture • Appropriate controls • A priori definition of “best practice” • Links to other initiatives • Specific audit recommendations • Delineation of the research gap