Download
1 / 36
360 likes | 1.01k Views
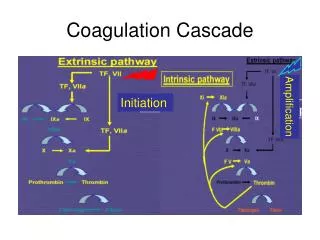
COAGULATION EMERGENCIES. How to deal with/avoid a bloodbath. COAGULATION EMERGENCIES. Congenital Coagulation Abnormalities Hemophilia Von Willebrand disease ITP Dilutional Coagulopathy Massive Medical/Surgical Bleeding TTP/HUS Acquired Bleeding/Clotting Disorders Inhibitors . Case 1.

E N D
COAGULATION EMERGENCIES How to deal with/avoid a bloodbath
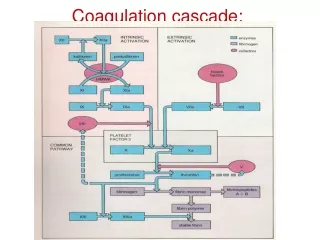
COAGULATION EMERGENCIES • Congenital Coagulation Abnormalities • Hemophilia • Von Willebrand disease • ITP • Dilutional Coagulopathy • Massive Medical/Surgical Bleeding • TTP/HUS • Acquired Bleeding/Clotting Disorders • Inhibitors
Case 1 • 27 year old man, known mild hemophilia B, presents to ER with massive GI bleed. 2 days previously had been placed on Naproxen for a twisted knee.
HEMOPHILIA • Mild - > 5% activity; bleeding only with trauma or surgery • Moderate – 1-5% activity - Bleeding with minor trauma; occasional spontaneous hemarthroses • Severe - < 1% activity – Spontaneous hemarthroses & soft tissue bleeds
HEMOPHILIA – General Rules RE: Rx • Treat first; ask questions later • Bleeding into closed spaces stops!! • AVOID EMERGENT PROCEDURES IF POSSIBLE • No procedures without replacement Rx • Avoid weekend/night procedures • No procedures without Hematology & Lab backup
INITIAL Rx OF HEMOPHILIA A Usual Product: Monoclonal Purified F VIII
INITIAL Rx OF HEMOPHILIA B Usual Product: Recombinant or Monoclonal F IX
Case 2 • 42 year old man presents with swollen, markedly inflamed. Knee tapped 3 days previous; Dx gout. Then told MD – “By the way, I have von Willebrand disease.” Put on colchicine with initial improvement, but then knee acutely worse; retap showed frank blood.
VON WILLEBRAND DISEASE • Autosomal Dominant inheritance with variable penetrance • Distinct variability in severity even within same family • Lack of von Willebrand Factor causes • Decreased Factor VIII Activity • Defect in Platelet Adhesion
VON WILLEBRAND DISEASEClassification • Type I – Quantitative Defect • Type II – Qualitative Defect • Type IIa – No multimer formation • Type IIb – Decreased multimers, decreased platelets • Type IIc – Other Protein Defects • Type IIn – Defect in Factor VIII Binding • Type III – Severe Quantitative Defect
VON WILLEBRAND DISEASETreatment • DDAVP – Releases vWF from stores • 70% respond; must test prior to use in critical situation • Humate-P – Factor VIII concentrate rich in vWF; approved for Rx of vWD • Dosage: 60-80 units/kg initial dose • Cryoprecipitate – Gold standard; 40 units/kg for 0-100% of normal; ½ life 12-24 hours
Case 3 • 28 year old woman, previously healthy, who comes in with sudden onset of petechial rash and heavy menses; No medications. Platelet count in ER 2,000/microliter; Hgb 12.5 g/dl
IMMUNE THROMBOCYTOPENIA PURPURA • IgG mediated • Platelets removed by macrophages • Antibodies can act on marrow as well • No good diagnostic test
ITP • Generally chronic illness in adults • Patients often tolerate very low platelet counts • AVOID PLATELET TRANSFUSIONS unless bleeding significantly • If significant bleeding, need to be treated urgently
ITP - Treatment • Focus on inhibiting macrophage activity • Corticosteroids • High Dose IVIg • IV Rhogam (anti-D) – For Rh Positive patients only – Causes mild hemolytic anemia • Splenectomy – For actively bleeding patients
Case 4 • 56 year old woman s/p mitral valve replacement for 2nd time 2 hours ago; on cardiopulmonary bypass 3½ hours; now bleeding from chest tubes > 500 ml/hour, & no clot formation in tubes. Blood pressure OK on low dose pressors; has received 12 units of platelets and 8 units of FFP, without effect
DILUTIONAL COAGULOPATHYUsual Causes • Post-operative bleeding, esp post-bypass • Variceal bleeding • Major trauma • Aortic aneurysm • Obstetrical emergencies
DILUTIONAL COAGULOPATHY • Generally need to lose 1½-2 blood volumes before invoking this • Cannot tell bleeding from low platelets from bleeding from coagulopathy or from surgical bleeding • Critical to determine cause before committing large amounts of blood products • Treatment should be guided by lab results
DILUTIONAL COAGULOPATHY • Most important tests: PT, Plt, Fibrinogen • Goal is to correct to hemostatic values, NOT to normal • Hemostatic values generally 30% of normal clotting factor levels • PT < 20-21 seconds • aPTT < 50 seconds • Plt > 50,000 • Fibrinogen > 100
DILUTIONAL COAGULOPATHY • Products to use: • Platelets – 6 units will raise count by 50,000 • FFP – 4-6 units will raise all clotting factors by 25-30% (in normal sized adult) • Cryoprecipitate – 10 units will raise fibrinogen by 100 mg/dl • 6 units FFP has fibrinogen of 12 units of cryoprecipitate • GIVE PRODUCTS RAPIDLY!!! • DDAVP usually not useful • Amicar may be helpful if no evidence of DIC
DILUTIONAL COAGULOPATHYSpecial Circumstances • Aspirin – May be able to use small doses of platelets • Coumadin/Vitamin K deficiency – Often need more FFP & definitely need Vitamin K • Heparin – Reverse with protamine • Uremia – Cryoprecipitate will help improve platelet function • IIb/IIIa inhibitors – All platelets dysfunctional; start with 12 units platelets • Obstetrical emergencies – DIC until proven otherwise; correct fibrinogen early
Case 5 • 48 year old man, Hx diabetes, hypertension, drug abuse, admitted with 3 days of fever & confusion. Bloods in ER show Hgb 7.5 (normal 14.5 for him), platelets 12,000; Coombs negative. Blood smear shows schistocytes; creatinine 1.6, LD 540, Bili 4.5/0.8
TTP • Rare but important disease entity • Sporadic & relapsing form • Caused by congenital defect of &/or antibody against vWF-cleaving metalloproteinase • Drugs also important • Calcineurin inhibitors • Ticlopidine/Clopidogrel • Universally fatal without treatment • With treatment > 90% survival, usually without sequelae
TTP • Microangiopathic hemolytic anemia – Blood smear is critical to assess • Thrombocytopenia • Mental status changes • Fever • Renal insufficiency • DO NOT SEE coag abnormalities!
TTP – Differential Diagnosis • DIC • HUS • Lupus vasculitis • Malignant hypertension • HEELLP syndrome (pregnancy only) • Transplant rejection
TTP - Treatment • Corticosteroids • Plasmapheresis/Plasma Exchange • Easier to manage fluids • Replaces missing metalloproteinase • Removes antibody to metalloproteinase • Vincristine, Splenectomy, Rituximab – For refractory cases • Aggressive – 1.5-2 plasma volume exchanges daily; sometimes need to continue x weeks • Survival > 90%; sequelae minimal if begun early
Case 6 • 65 year old man admitted with chest pain; EKG shows non-Q wave MI, & went to cath lab for cath & stent placement. Post-procedure, echo shows LV thrombus in apex. Rx with Lovenox starting 5 days later; platelet count fell from 300,000 to 35,000 over 1 day
Heparin-Induced Thrombocytopenia • Immunologic reaction • Occurs 5-10 days post- initial exposure to heparin • Usually not associated with bleeding • 5-10% associated with thrombosis at presentation • Of those without thrombosis, 50% will develop thrombosis within 14 days
Heparin-Induced Thrombocytopenia • Cause of thrombosis: Platelet aggregation • Coumadin alone, esp in large doses, runs risk of venous gangrene • Need parenteral agent along with Coumadin • Lepirudin – Hirudin derivative • Argatroban – Small molecule thrombin inhibitor
Case 7 • 75 year old woman, Hx paroxysmal A fib, fell & suffered intertrochanteric fracture of L hip. Brought to ER @ 5:30 pm; scheduled for surgery in AM; aPTT 55 seconds. Only meds digoxin & naproxen. No prior Hx of bleeding; only has bruise over fractured hip
ACQUIRED COAGULATION INHIBITORS – Lupus Anticoagulant • Antiphospholipid antibody • Laboratory rather than clinical anticoagulant • Test by looking for presence of anticoagulant in assay where amount of phospholipid is rate-limiting step • Causes prothrombotic rather than antithrombotic condition
Case 8 • 92 year old woman brought to ER by family because of a large spontaneous ecchymosis on her R neck. Admission labs were normal except for an aPTT of 70 seconds (normal 25-35 seconds)
ACQUIRED COAGULATION INHIBITORS • 80-90% are associated with hemophilia patients, mostly hemophilia A • Most of the rest are associated with lymphoproliferative disorders • Most commonly directed against factor VIII • Typically low titer, high affinity, slow-binding antibodies, usually IgG • Marked decrease in the survival of transfused product • Commonly have MAJOR bleeding problems
ACQUIRED COAGULATION INHIBITORS • Test by mixing patient’s plasma with normal plasma, incubating x 1 hour @ 37°, and then measuring the time it takes to clot. If time post-incubation is > 5 seconds longer than the control time, presence of inhibitor to a clotting protein • Then must determine the protein against which inhibitor is directed • Occasionally have false positive lupus anticoagulant assays
ACQUIRED COAGULATION INHIBITORS - Treatment • Acute – to stop bleeding • FEIBA (Factor Eight Inhibitor Bypass Activity), or Autoplex – 40 units/kg • High Risk of Thromboembolic Disease • Porcine Factor VIII • Recombinant Factor VIIa – Reserved for FEIBA failures and/or surgery • Chronic – To decrease antibody titer • Steroids • Rituximab • Cyclophosphamide, Azathioprine • Malmö Protocol (Induction of Immune Tolerance) • 25-50% mortality even with optimal treatment