Download
1 / 18
190 likes | 261 Views
A fantastic selection of posters and resources I have amalgamated into a slideshow. ALL CREDITS ICS<br><br>The Intensive Care Society is delighted to share THE new wellbeing resource pack developed with Dr Julie Highfield, Clinical Psychologist. ICS poster series aims to improve our understanding of psychological wellbeing at work, the impact reduced wellbeing can have and what we can do in response, and includes tips for dealing with extraordinary situations such as COVID-19 and everyday working in critical care. <br><br>It prompts the reader(s) to consider:<br><br>Tips for approaching self-care<br>How to manage personal wellbeing<br><br> improve our workplace<br>When to ask for help

E N D
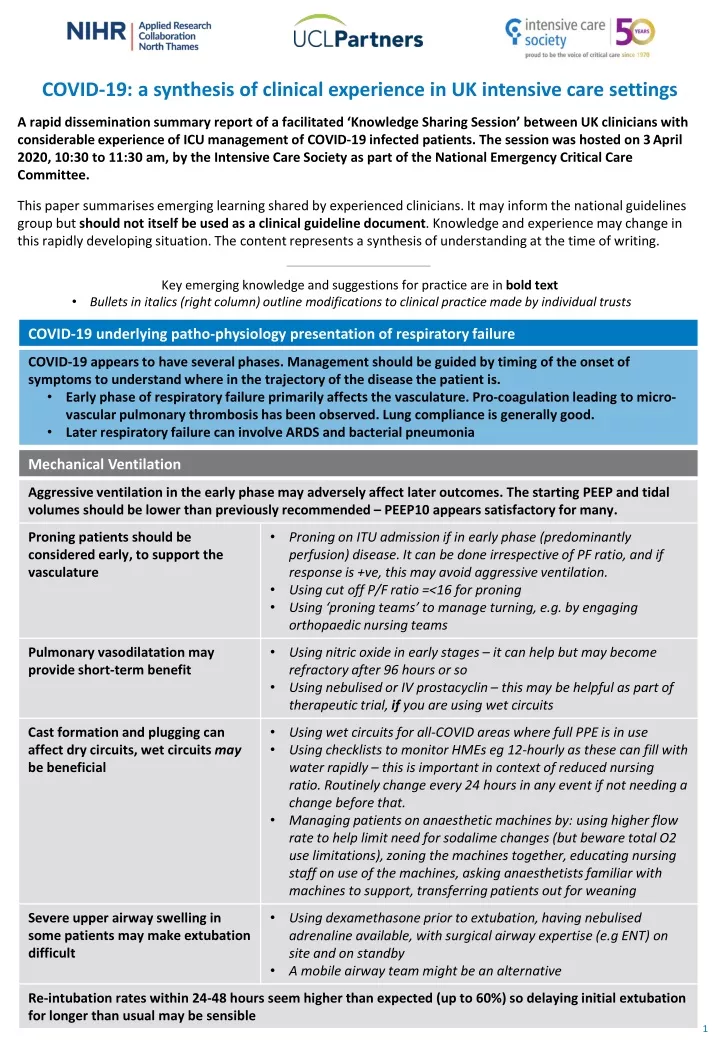
COVID-19: a synthesis of clinical experience in UK intensive care settings A rapid dissemination summary report of a facilitated ‘Knowledge Sharing Session’ between UK clinicians with considerable experience of ICU management of COVID-19 infected patients. The session was hosted on 3April 2020, 10:30 to 11:30 am, by the Intensive Care Society as part of the National Emergency Critical Care Committee. This paper summarises emerging learning shared by experienced clinicians. It may inform the national guidelines group but should not itself be used as a clinical guideline document. Knowledge and experience may change in this rapidly developing situation. The content represents a synthesis of understanding at the time of writing. Key emerging knowledge and suggestions for practice are in bold text Bullets in italics (right column) outline modifications to clinical practice made by individual trusts • COVID-19 underlying patho-physiology presentation of respiratory failure COVID-19 appears to have several phases. Management should be guided by timing of the onset of symptoms to understand where in the trajectory of the disease the patient is. • Early phase of respiratory failure primarily affects the vasculature. Pro-coagulation leading to micro- vascular pulmonary thrombosis has been observed. Lung compliance is generally good. • Later respiratory failure can involve ARDS and bacterial pneumonia Mechanical Ventilation Aggressive ventilation in the early phase may adversely affect later outcomes. The starting PEEP and tidal volumes should be lower than previously recommended – PEEP10 appears satisfactory for many. • Proning patients should be considered early, to support the vasculature Proningon ITU admission if in early phase (predominantly perfusion) disease. It can be done irrespective of PF ratio, and if response is +ve, this may avoid aggressive ventilation. Using cut off P/F ratio =<16 for proning Using ‘proning teams’ to manage turning, e.g. by engaging orthopaedic nursing teams • • • Pulmonary vasodilatation may provide short-term benefit Using nitric oxide in early stages – it can help but may become refractory after 96 hours or so Using nebulised or IV prostacyclin – this may be helpful as part of therapeutic trial, if you are using wet circuits • • • Cast formation and plugging can affect dry circuits, wet circuits may be beneficial Using wet circuits for all-COVID areas where full PPE is in use Using checklists to monitor HMEs eg 12-hourly as these can fill with water rapidly – this is important in context of reduced nursing ratio. Routinely change every 24 hours in any event if not needing a change before that. Managing patients on anaesthetic machines by: using higher flow rate to help limit need for sodalime changes (but beware total O2 use limitations), zoning the machines together, educating nursing staff on use of the machines, asking anaesthetists familiar with machines to support, transferring patients out for weaning • • Severe upper airway swelling in some patients may make extubation difficult Using dexamethasone prior to extubation, having nebulised adrenaline available, with surgical airway expertise (e.g ENT) on site and on standby A mobile airway team might be an alternative • Re-intubation rates within 24-48 hours seem higher than expected (up to 60%) so delaying initial extubation for longer than usual may be sensible 1
Fluid Balance Careful use of fluids towards euvolaemia may be beneficial in early phase disease - provided that the ventilation effort is well controlled to avoid oedema – as perfusion is a problem and prior to ITU patients tend to have been kept dry. Antibiotics • Antibiotic usage should be judicious. There are some reports of later aspergillosis and candida infections. Stopping antibiotics in COVID patients unless clearly indicated, using procalcitonin (PCT) and other inflammatory markers to monitor for bacterial infection and restarting as required* Using procalcitonin as a ‘stop’ signal to guide when to stop antibiotic use* • *False negative PCTs seem less of an issue than false positives in determining antibiotic use – anecdotally, rising procalcitonin has also been seen in patients without evidence of bacterial infection, perhaps in relation to ‘cytokine storm’, and so a low PCT may be more helpful (true negative) than a high PCT (false positive) Workforce and Infection Control • Ensure staff are comfortable in their PPE Buddying for donning and doffing, potentially using medical students to observe and confirm effective practice • Promote effective use of the Teams model (eg for resus, intubation, proning) Developing SOPs for tasks for helpers – links to some resources which can be adapted for local use are available below • Beware of ‘cognitive overload’ which can detract from getting basic ITU care right Having a tactical commander on site so the clinical leads can focus on clinical tasks and provide support to the nursing and allied staff Renal Support Renal injury has been more common in UK cases than anticipated (20-35% of ITU patients). Careful attention to adequate hydration, and use of lower PEEP, may help. • Consider commencing therapeutic anticoagulation prior to haemofiltration Using aPTT for monitoring, and close partnership with renal team to manage resources Using shorter sharper diafiltrating to service machines to more than 1 person and manage filter supply • Oxygen While this is a national issue and work is underway, it will be necessary to work with your local oxygen engineering team to understand the limitations of your local system Regionally – consider the use of oxygen around your local area when considering logistics of transport, mutual aid, patient transfers, etc Additional resources • British Association of Critical Care Nurses: https://www.baccn.org/about/covid-19-nurse-educational- resource-centre/resources-1/ • NHS England and NHS Improvement: https://www.england.nhs.uk/coronavirus/secondary-care/ 2
With thanks to our panel members Andre Vercueil, King's College Hospital Brijesh Patel, Royal Brompton and Harefield NHS Foundation Trust Daniel Martin, Royal Free Hospital Ganesh Suntharalingam, Northwick Park Hospital, Intensive Care Society Hugh Montgomery, Whittington Hospital, Intensive Care Society Luigi Camporota, Guy's and St Thomas' Hospital NHS Foundation Trust Mark Hamilton, St George's Hospital Mike Grocott, University Hospital Southampton NHS Foundation Trust Nicki Credland, British Association of Critical Care Nurses (BACCN) Ramani Moonesinghe, National Clinical Director for Critical Care, NHS England/NHS Improvement Shahana Uddin, King's College Hospital Tamas Szakmany, Royal Gwent Hospital Contact details The Intensive CareSociety www.ics.ac.uk info@ics.ac.uk +44 (0)2072804350 Report written by Dr NiranRehill, Public Health Specialist, NIHR ARC North Thames; Designed by Morgan McKean, Communications and Engagement Manager, UCLPartners
HOW TO APPROACH SELF-CARE Your health and wellbeing matter. In the context of working in a busy critical care unit the following may be helpful. Self-awareness is important There will always be that one case that has a greater impact, often because there is something that you connect to. Be aware of the things that may bother you, and your own warning signs of stress. General self-care Take time for the things that bring you rest and joy. Self-compassion and embrace uncertainty Beware your own critical eye. Working in healthcare is hard and there are times when you will feel there is nothing you can do, or you cannot control the situation. Be kind to yourself and your colleagues. There are times when our psychological wellbeing is so challenged that self-care is not enough. If you are finding things difficult, consider talking to your line manager or someone you trust about the impact of your work. You may want a referral to your local employee wellbeing service. www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
IMPROVING OUR WORKPLACE Critical care is a challenging environment to work in, however there are things that help reduce the emotional impact of the work. The following are ideas for your teams. Creating space for the team to get together Creating opportunities to discuss the impact of cases such as Reflective Rounds can help staff process the traumatic impact of the work. Safety huddles, simulation and quality and safety meetings allow a structured way of spending time together and learning more about each other. Informal spaces such as staff rooms and social events also help. ✔ ✔ ✔ Design the working day well The working day should be organised to balance demands but should also provide positive experiences with patients and families. Engage staff Create ways to engage your team, from team meetings and listening to ideas, to engaging junior staff with projects to help their sense of belonging. Have you noticed changes in your team? Why not have a conversation? Don’t be afraid to ask, ‘are you ok?’ www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
IMPROVING OUR WORKPLACE Critical care is a challenging environment to work in, however there are things that help reduce the emotional impact of the work. The following are ideas for your teams. ✘ ✔ Increase civility @?!**! We know rudeness increases clinical error. Although we can all become stressed in this environment we should beware of creating a permissive environment for rudeness to thrive. Look at the Civility Saves Lives campaign. Learning ✔ Encourage learning through excellence and try creating protected learning time. It’s important to manage a mistake through ‘what went wrong?’ not ‘who went wrong?’ For more information: Look at the Just Culture campaign. Developing leaders A good leader has developed strong sense of emotional intelligence and self-awareness. Encourage new leaders to engage in leadership development to include coaching and 360° appraisals. Have you noticed changes in your team? Why not have a conversation? Don’t be afraid to ask, ‘are you ok?’ www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
IMPROVING OUR WORKPLACE Critical care is a challenging environment to work in, however there are things that help reduce the emotional impact of the work. The following are ideas for your teams. Creating space for the team to get together Creating opportunities to discuss the impact of cases such as Reflective Rounds can help staff process the traumatic impact of the work. Safety huddles, simulation and quality and safety meetings allow a structured way of spending time together and learning more about each other. Informal spaces such as staff rooms and social events also help. ✔ ✔ ✔ Design the working day well The working day should be organised to balance demands but should also provide positive experiences with patients and families. Engage staff Create ways to engage your team, from team meetings and listening to ideas, to engaging junior staff with projects to help their sense of belonging. Have you noticed changes in your team? Why not have a conversation? Don’t be afraid to ask, ‘are you ok?’ www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
IMPROVING OUR WORKPLACE Critical care is a challenging environment to work in, however there are things that help reduce the emotional impact of the work. The following are ideas for your teams. ✘ ✔ Increase civility @?!**! We know rudeness increases clinical error. Although we can all become stressed in this environment we should beware of creating a permissive environment for rudeness to thrive. Look at the Civility Saves Lives campaign. Learning ✔ Encourage learning through excellence and try creating protected learning time. It’s important to manage a mistake through ‘what went wrong?’ not ‘who went wrong?’ For more information: Look at the Just Culture campaign. Developing leaders A good leader has developed strong sense of emotional intelligence and self-awareness. Encourage new leaders to engage in leadership development to include coaching and 360° appraisals. Have you noticed changes in your team? Why not have a conversation? Don’t be afraid to ask, ‘are you ok?’ www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
MANAGING YOUR WELLBEING Striking a balance between the positive factors and resources at work and the negative factors or demands at work isn’t always easy. It is normal to have difficult days, but the following can help: Effective “rollercoaster riding” Some people describe working in critical care as an emotional rollercoaster, so ways to counter this are important. Remember to take your breaks. Create a few minutes to step away from the unit, take a breath and relax. Outside of work allow enough “down time” where you can switch off. Acknowledge you are only human The clinical work can provoke strong emotions. Sometimes when you have other issues outside work, coping with those emotions can feel even harder. Space to reflect, share and beware using avoidant coping strategies We see a lot in critical care, and we need space to reflect and make sense of this. Keeping very busy, avoiding discussing things, over-eating, and drinking to excess are all risk factors. Your support networks inside and outside work are good places to discuss the day. There are times when our psychological wellbeing is so challenged that self-care is not enough. If you are finding things difficult, consider talking to your line manager or someone you trust about the impact of your work. You may want a referral to your local employee wellbeing service. www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
AM I OK Do you regularly feel DISCONNECTED from the relationship of caring for the patient, family, and colleagues? 1 Do you regularly feel EMOTIONAL EXHAUSTION - like you have nothing left to give? 2 Do you regularly feel A LACK OF FEELING OF ACCOMPLISHMENT or feelingINEFFECTIVE in what you do? 3 If you answered YES to all three, consider talking to your line manager or someone you trust about the impact of your work. You may want a referral to your local employee wellbeing service. www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
ADVICE FOR SUSTAINING STAFF WELLBEING IN CRITICAL CARE DURING AND BEYOND COVID-19 The anticipated needs of staff will vary across each of the phases, consider the following support mechanisms: Phases Issues and likely impact Needs and recommended approach Pre-phase: Anticipatory anxiety about what’s on its way. Increase a sense of control - the team are in a safe pair of hands. Inability to think clearly, feeling overwhelmed, planning. Reassurance and planning. No cases on unit Communication errors. Communication updates are key (you may be thinking ahead, they are thinking now). Tension in working relationships. Escalation plan. “Readiness” burnout. Support to managers who are making plans and holding the stresses. Initial phase: Case 1 Starting to get going, lots of trying out, lost time, repetition and frustration. War room - planning central to allow centralised communication. Further anticipatory anxiety Management are visible and available. Regular communication bulletins and open forums. Core Phase: Full scale -Multiple cases Biggest risk period. Have runners in PPE areas. Fear infection and implications for families. Promote peer support. Overwhelming workload. It’s okay to say you are not okay - Senior staff to model this. Full go mode- adrenalin and automatic pilot. Rotate workers from high-stress to lower-stress functions. Exhaustion. Moral distress as healthcare rationed. Small pre-brief and debrief the day. Distress linked to personal or family experience of COVID-19. Partner inexperienced workers with their more experiences colleagues. Experience fear or stigma when out in public. Psychological first aid - drop in sessions for staff with employee wellbeing if you have it. Ensure the basics: Breaks, Facilities (food trolley in staff room), Sleep, Days off. Manage visitors End Phase: Immediate aftermath Exhaustion and post trauma recovery / stress Debriefing. Staff 1-1 and group sessions. Learning and preparation for the future. Organise thanks and reward. Look out for signs of PTSD in staff: • on edge and hyper arousal, poor sleep • flashbacks or re-experiencing • avoidance of reminders. Long term Some ongoing PTSD Reflection and learning www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
SELF-CARE DURING COVID-19 Most importantly this is unprecedented: It is okay to not be okay • Seek information updates at specific times during the day once or twice. The sudden and near-constant stream of news reports can cause anyone to feel worried. Get the facts. www.gov.uk • Feeling stressed is an experience that you and many of your colleagues are likely going through. It is normal to be feeling this way in the current situation. Stress and the feelings associated with it are by no means a reflection that you cannot do your job or that you are weak. • Managing your stress/psychosocial wellbeing during this time is as important as managing your physical health. • Take care of your basic needs and ensure rest and respite during work or between shifts, eat sufficient and healthy food, engage in physical activity, and stay in contact with family and friends. • This is an unprecedented scenario, don’t try to learn new strategies, use the ones that you have used in the past to manage times of stress. • This is likely to be a marathon - pace yourself • Consider your psychological energy levels - you will need to “fill up” after “emptying the tank” • Be aware of your “bandwidth”- it might take longer to think things through and make sense of things if you are feeling overwhelmed • Beware dramatic language that might panic your colleagues. • Avoid using unhelpful coping strategies such as tobacco, alcohol or other drugs. • Some workers may unfortunately experience avoidance by their family or community due to stigma or fear. If possible, staying connected with your loved ones including through digital methods is one way to maintain contact. Turn to your colleagues or team leader for social support - your colleagues may be having similar experiences to you. STOP, BREATHE, then THINK- slowing your breathing slows the stress cycle and re-engages your frontal lobes - then you can think. www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
ADVICE FOR SUSTAINING STAFF WELLBEING IN CRITICAL CARE DURING AND BEYOND COVID-19 The anticipated needs of staff will vary across each of the phases, consider the following support mechanisms: Phases Issues and likely impact Needs and recommended approach Pre-phase: Anticipatory anxiety about what’s on its way. Increase a sense of control - the team are in a safe pair of hands. Inability to think clearly, feeling overwhelmed, planning. Reassurance and planning. No cases on unit Communication errors. Communication updates are key (you may be thinking ahead, they are thinking now). Tension in working relationships. Escalation plan. “Readiness” burnout. Support to managers who are making plans and holding the stresses. Initial phase: Case 1 Starting to get going, lots of trying out, lost time, repetition and frustration. War room - planning central to allow centralised communication. Further anticipatory anxiety Management are visible and available. Regular communication bulletins and open forums. Core Phase: Full scale -Multiple cases Biggest risk period. Have runners in PPE areas. Fear infection and implications for families. Promote peer support. Overwhelming workload. It’s okay to say you are not okay - Senior staff to model this. Full go mode- adrenalin and automatic pilot. Rotate workers from high-stress to lower-stress functions. Exhaustion. Moral distress as healthcare rationed. Small pre-brief and debrief the day. Distress linked to personal or family experience of COVID-19. Partner inexperienced workers with their more experiences colleagues. Experience fear or stigma when out in public. Psychological first aid - drop in sessions for staff with employee wellbeing if you have it. Ensure the basics: Breaks, Facilities (food trolley in staff room), Sleep, Days off. Manage visitors End Phase: Immediate aftermath Exhaustion and post trauma recovery / stress Debriefing. Staff 1-1 and group sessions. Learning and preparation for the future. Organise thanks and reward. Look out for signs of PTSD in staff: • on edge and hyper arousal, poor sleep • flashbacks or re-experiencing • avoidance of reminders. Long term Some ongoing PTSD Reflection and learning www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
SELF-CARE DURING COVID-19 Most importantly this is unprecedented: It is okay to not be okay • Seek information updates at specific times during the day once or twice. The sudden and near-constant stream of news reports can cause anyone to feel worried. Get the facts. www.gov.uk • Feeling stressed is an experience that you and many of your colleagues are likely going through. It is normal to be feeling this way in the current situation. Stress and the feelings associated with it are by no means a reflection that you cannot do your job or that you are weak. • Managing your stress/psychosocial wellbeing during this time is as important as managing your physical health. • Take care of your basic needs and ensure rest and respite during work or between shifts, eat sufficient and healthy food, engage in physical activity, and stay in contact with family and friends. • This is an unprecedented scenario, don’t try to learn new strategies, use the ones that you have used in the past to manage times of stress. • This is likely to be a marathon - pace yourself • Consider your psychological energy levels - you will need to “fill up” after “emptying the tank” • Be aware of your “bandwidth”- it might take longer to think things through and make sense of things if you are feeling overwhelmed • Beware dramatic language that might panic your colleagues. • Avoid using unhelpful coping strategies such as tobacco, alcohol or other drugs. • Some workers may unfortunately experience avoidance by their family or community due to stigma or fear. If possible, staying connected with your loved ones including through digital methods is one way to maintain contact. Turn to your colleagues or team leader for social support - your colleagues may be having similar experiences to you. STOP, BREATHE, then THINK- slowing your breathing slows the stress cycle and re-engages your frontal lobes - then you can think. www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
UNDERSTANDING PSYCHOLOGICAL WELLBEING AT WORK Wellbeing is the achievement of satisfaction in absence of sustained distress, with a sense of control, meaning, and purpose, and the ability to maintain good relationships. Psychological wellbeing in the workplace is multi- faceted and influenced by individual differences (such as personality and coping style) but also work factors such as: Work factors that can influence Psychological wellbeing relationships job design team attitudes ethos of the wider organisation management and leadership style colleagues How are the above factors within your critical care unit? Positive changes in any of the areas can result in better psychological wellbeing for all of the team. www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
IMPACT OF REDUCED WELLBEING Psychological stress is defined as demands exceeding resources. Small amounts of stress may be perceived as challenging and motivating, however sustained and excessive stress may lead to psychological distress such as feeling pressured and being overwhelmed. Extreme stress can result in insomnia irritability anxiety burnout fatigue traumatic stress depression We all have a limited capacity - stresses at home make it harder to manage stresses at work, and vice versa. If you are experiencing any of the above consider talking to your line manager or someone you trust about the impact of your work. You may want a referral to your local employee wellbeing service. www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
UNDERSTANDING PSYCHOLOGICAL WELLBEING AT WORK Wellbeing is the achievement of satisfaction in absence of sustained distress, with a sense of control, meaning, and purpose, and the ability to maintain good relationships. Psychological wellbeing in the workplace is multi- faceted and influenced by individual differences (such as personality and coping style) but also work factors such as: Work factors that can influence Psychological wellbeing relationships job design team attitudes ethos of the wider organisation management and leadership style colleagues How are the above factors within your critical care unit? Positive changes in any of the areas can result in better psychological wellbeing for all of the team. www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care
IMPACT OF REDUCED WELLBEING Psychological stress is defined as demands exceeding resources. Small amounts of stress may be perceived as challenging and motivating, however sustained and excessive stress may lead to psychological distress such as feeling pressured and being overwhelmed. Extreme stress can result in insomnia irritability anxiety burnout fatigue traumatic stress depression We all have a limited capacity - stresses at home make it harder to manage stresses at work, and vice versa. If you are experiencing any of the above consider talking to your line manager or someone you trust about the impact of your work. You may want a referral to your local employee wellbeing service. www.ics.ac.uk Author: Dr Julie Highfield, Consultant Clinical Psychologist, Cardiff Critical Care