1 / 39
430 likes | 863 Views
Introduction, Definition, Etiology, Transmission, Epidemiology, Treatment, Control and prevention

E N D
INFECTIOUS DISEASES I (Bacterial Diseases) ANTHRAX Faculty of Veterinary Medicine & Animal Husbandry Somali National University Mogadishu, Gaheyr Campus Feb. 24. 2020
Sverdlovsk, Russia, 1979 • 94 people sick – 64 died • Soviets blamed contaminated meat • Denied link to biological weapons • 1992 • President Yeltsin admits outbreak related to military facility • Western scientists find victim clusters downwind from facility • Caused by faulty exhaust filter
South Africa, 1978-1980 • Anthrax used by Rhodesian and South African apartheid forces • Thousands of cattle died • 10,738 human cases • 182 known deaths • Black Tribal lands only
Tokyo, 1993 • Aum Shinrikyo • Japanese religious cult • “Supreme truth” • Attempt at biological terrorism • Released anthrax from office building • Vaccine strain used • No human injuries Center for Food Security and Public Health, Iowa State University, 2011
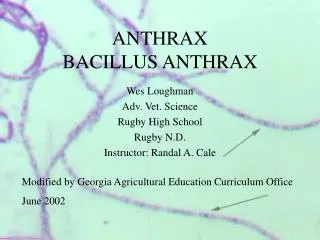
Definition • Is an infectious, usually fatal disease of warm-blooded animals, especially of cattle and sheep, caused by the bacterium Bacillus anthracis. • It is one of the oldest recorded diseases in both humans and animals (Zoonotic). • Robert Koch discovered the causal organism of the anthrax and the development of the infection.
Importance • Anthrax is a serious zoonotic disease that can affect most mammals and several species of birds, but is particularly important in herbivores • The disease can be endemic or epizootic and can kill large number of animals (500) and environmental problems. • Bioterrorist attack
Etiology • Bacillus anthracisis aerobic or facultative anaerobic,Gram-positive typically rod shaped, non-motile, spore forming bacteria. • The shape of the bacilli in body fluids is square like a brick but has rounded edges when in cultures. • In tissue fluids it has a well defined capsule which is responsible for the virulence.
The spores are formed under suitable environmental conditions but never found in the animals’ body. • Colonieshave irregular margins in nutrient agar which give the colonies the so called medusa head appearance.
B. anthracisproduces a tripartite extracellular toxin consisting of three protein components known as: The oedema factor (EF) The protective antigen (PA) The lethal factor (LF)
Vegetative cells of B. anthracis are not resistant to adverse environmental conditions, while the spores are very resistant and can resist the physical and chemical agents. • Spores may persist in soil for decades and withstand humid heat at 120˚C for 10 minutes and dry heat at 160˚C for more than 1 hour.
Occurrence • Although B. anthracis can be found worldwide, anthrax cases usually occur only in limited geographic regions. • Outbreaks are most common in areas characterized by alkaline and warm environment, and periodic episodes of flooding • It is common in some parts of Africa, Asia, the Middle East and the USA.
Distribution 20,000 to 100,000 cases estimated globally/year http://www.vetmed.lsu.edu/whocc/mp_world.htm
Susceptible Animals • All mammals as well as some birds and reptiles are susceptible to Bacillus anthracis infection. • It is an infection of herbivores especially cattle and small ruminants which ingest the pathogens as spores or vegetative forms from the soil. • Buffaloes and camels are also susceptible but pigsrarely become infected and carnivores only exceptionally • Adults being more susceptible than the young animals.
Source of infection • Vegetative bacilli are disseminated by sick animals in large amounts from their body openings or released from slaughtered or dead carcasses which can sporulate in and at soil at temperatures of 20-32˚C. • Buried carcasses can remain a source of infection for years because of spores which reach the animal through plants or ground water. • In rainy season the infection also increased due to the suitable environmental condition
Transmission • Pulmonary infection by inhalation of dust from the contaminated soil or from feed concentrate • By ingestion of contaminated feed of animal origin (carcass, bone and blood meal) when used in intensive animal production system. • Scavenger birds and carnivores are able to spread the infection over wide areas without getting infected themselves
Insects may spread the infection because B. anthracismay found in their excreta. • In humans the pathogens may enter aerogenically, cutaneously and enterically as vegetative forms or spores when contact with sick animals, diseased animals which have been slaughtered, animal products or carcasses of infected animals. • Entry through skin lesions in animals has not been ruled out
Pathogenesis • After infection, spores germinate and form encapsulated vegetative cells which produce toxin. • Bacilli are transported via lymphatics to regional lymph nodes where further multiplication takes place and from where vegetative bacilli continuously enter the blood stream and bacteraemia occurs.
The three different factors of toxin have different effects. • They react differently in different combinations.
Clinical signs Per acute • The incubation period may be less than 12 hours. • Animals die without showing any symptoms. • Only secretion of tar-like blood from mouth, nostril and anus.
Acute • The course lasts in 2-3 days. • Fever (42˚C) recumbence with severe disturbances of the circulation and respiration, haemorrhages in mucous membranes, loss of appetite. • Milk production decreased and pregnant animals usually abort. • Tar-like blood from body openings. • Bacillifound in large amounts in circulating blood and can be recognized from the typical capsule.
Chronic • Extend for more than 3 days before either recovery or death occur. • The most frequent sign is an oedematous swelling of the throat and the neck (pharynx and lymph nodes). • The infection may remain localized or progress to fatal septicaemia. • Usually occurs as a consequence of accidents in vaccination with Pasteur vaccine.
Day 6 Day 2 Day 4 Day 6 Day 10 Center for Food Security and Public Health, Iowa State University, 2011
Pathology • Tar-like bloodfrom body openingsdoesn’t clot at all or poorly clotted • The development of rigor mortis is incomplete • Enlargement of spleen which is the pathognomonic finding at necropsy. • Serosae are stained dark red • Extensive pulmonary oedema
Diagnosis • In endemic areas, symptoms and necropsy finding are helpful • Demonstration of B. anthracis by Giemsa stain or polychrome methylene blue in blood smears taken from the ear vessel in order to prevent opening of the carcass body fluids or tissues. • Isolation of the causative agent by culturing either from blood or internal organs. • Inoculation of experimental animals.
Molecular methods like PCR • Serologic tests like ELISA • A skin hypersensitivity test using Anthraxin
Treatment • The disease can be treated successfully if diagnosed in times with antibiotics and symptomatic treatment
Control • Good Management - Keep animals away from contaminated sites - Provide hygienic drinking water - Good stocking rate specially in the peak of the dry season - Maintenance of fodder reserves for the dry season - Using of sterilised feed or feed additives
Appropriate disposalof carcasses - By burning at the site where the animal died. But burning might lead to permanentcontamination of the pasture - Decontamination can help to prevent dissemination of the disease during outbreaks (in this case to prevent sporulation carcasses should not be opened and scavengers should also be prevented from accessing the carcass) - Deep burial may also be used but is less desirable
Vaccination with live vaccines such as: - Pasteur vaccine or Sterne -spore vaccine • Other appropriate measurements - Quarantines and isolation - Insect repellents help prevent flies from spreading the organism. - Prophylactic antibiotics are given to exposed and at-risk animals. - Grazing animals should be moved away from areas of possible contamination
Humans protected by preventing disease in animals • Veterinary supervision • Trade restrictions • Improved industry standards • Safety practices in laboratories • Post-exposure antibiotic prophylaxis
Cell-free filtrate • At risk groups • Veterinarians • Lab workers • Livestock handlers • Military personnel • Immunization series • Five IM injections over 18-week period • Annual booster