Download
1 / 44
0 likes | 38 Views
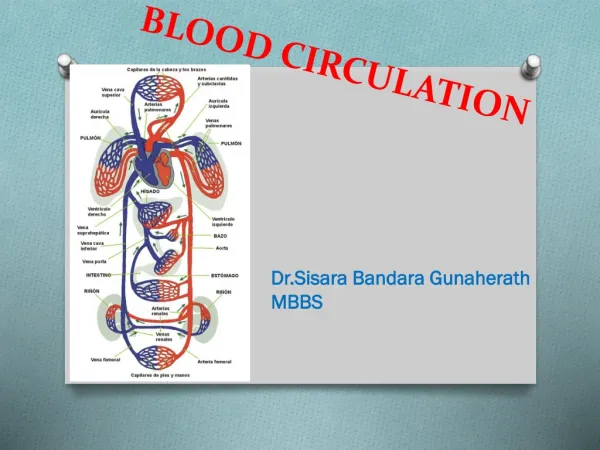
The circulatory system is made up of blood vessels that carry blood away from and towards the heart. Arteries carry blood away from the heart and veins carry blood back to the heart. The circulatory system carries oxygen, nutrients, and hormones to cells, and removes waste products, like carbon dioxide. Next, blood that returns to the heart has picked up lots of oxygen from the lungs. So it can now go out to the body. The aorta is a big artery that leaves the heart carrying this oxygenated blood. Branches off of the aorta send blood to the muscles of the heart itself.

E N D
Shri Shivaji Education Society, Amravati'sSHRI PUNDLIK MAHARAJ MAHAVIDYALAYA, NANDURA RLY. DIST. BULDANA Topic: Unit-I: Blood Circulation Class: B.Sc-III, Sem-V Mr. Shantaram Bhoye Assistant Professor & Head M.Sc., NET-JRF, SET, M.A.(Eng.)
Blood Circulation: Blood: • Blood is red colored fluid connective tissue. • It remains in fluid state till it is within the blood vessels. • The volume of blood in a normal adult is 5 liter. • Blood is slightly alkaline and its pH in normal conditions is 7.4. Constituents of blood: • Blood contains 8-9% blood cells and 91-92% liquid portion called as plasma. Blood Cells: • Red Cells: • Red Blood Cells or Erythrocytes • White Blood Cells or Leucocytes • Platelets or thrombocytes. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Red Blood Cells or Erythrocytes: • RBC are the non-nucleated formed elements in the blood. • The red color of the blood is due to the presence of Hb. • The RBC count ranges between 4 to 5.5 million per cubic millimeter of blood. • In adult males it is 5 millions/cu mm of blood and in adult female it is 4.5 millions/cu mm of blood. • Increase in the red blood cell count is called polycythemia. • Whereas, marked reduction in the red blood cell count is called anemia. Shape: • The RBC are disc shaped and biconcave (dumb bell shaped). • Crescentic shaped RBCs are found in sickle-cell anaemia. • Average life span of RBC is about 120 days. Erythrocytes Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Functions: • Transport of oxygen from lungs to the tissues. • Transport of Carbon dioxide from tissues to the lungs. • Hb in RBC acts as buffer and takes part in maintenance of acid-base balance. • RBC carry the blood group antigens. Ex. A-agglutinogen, B-agglutinogen and Rh-factor. These antigens help in determination of blood groups and blood transfusion. • Erythropoiesis is the process by which the, development and maturation of erythrocytes occur. Organs Producing RBC: • During pre-natal life liver, spleen and lymphoid organs and in adults red bone marrow produce RBC. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
White Blood Cells or Leucocytes: • These are the colorless and nucleated formed elements of blood. • They play important role in defense mechanism of the body. • Depending upon the presence or absence of granules in the cytoplasm the leucocytes are classified into two types. • Total WBC count varies from 4000 to 11,000/cu mm of blood. A. Granulocytes: a) Neutrophils: • Neutrophils have small granules in the cytoplasm. • The granules are violet in color. • The nucleus is multilobed. • The diameter of cell is 10 to 12 microns. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
b) Eosinophils: • Eosinophils have coarse (larger) granules which stain bright red or orange with eosin. • The nucleus is bilobed. • The diameter of the cell varies between 10-14 micrometer. c) Basophils: • Basophils also have larger granules in the cytoplasm. • The granules stain purple blue with basic dyes like methylene blue. • Nucleus is bilobed. • Diameter of the cell is 8-10 microns. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
B) Agranulocytes: • a) Monocytes: • These are the largest leucocytes with diameter of 14 to 18 microns. • The cytoplasm is clear without granules. • The nucleus is round, oval, horseshoe or kidney shaped. • The nucleus is either in the center of the or it is pushed to one side and a large amount of cytoplasm is seen. • b) Lymphocytes: • The lymphocytes have little amount of cytoplasm with a large, oval or kidney shaped nucleus occupying the whole cytoplasm. • 1) T-Lymphocytes-concerned with cellular immunity. • 2) B-Lymphocytes-concerned with humoral immunity. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Variation in WBC count: • 1. Leukopenia: Decrease in the total WBC count cause leucopenia. • 2. Eosinophilia: Increase in eosinophil count cause eosinophilia. • 3. Leukemia: The leukemia is the condition which occurs due to malignancy. It is associated with abnormal and uncontrolled increase in total WBC count. Functions of WBC: • 1. Neutrophils: • It is play important role in the defense of body. • The granules of neutrophils contain antibody like substance called defensins which are active against bacteria and fungi. • 2. Eosinophils: • The major functions of these cells are detoxification, disintegration and removal of foreign proteins. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
3. Basophils: • The basophils play an important role in the healing processes after inflammation and allergy. 4. Monocytes: • The monocytes are also motile and phagocytic. • They are precursors of tissue macrophages. • They play important role of the body. 5. Lymphocytes: • They play important role in immunity. • T-lymphocytes are responsible for the development of cellular immunity and B-lymphocytes are responsible for the development of humoral immunity (Major defensive mechanism against the bacterial infection). Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Platelets: • Platelets or thrombocytes are small colourless non nucleated cells. • These formed elements are considered to be the fragments of cytoplasm. • They are spherical or rod shaped. • Sometimes the platelets are of dumb bell, comma, cigar or any other unusual shape. • Normal platelets count is 2.5 lack/cu mm of blood. • Life span of platelets is 8-11 days. • Decrease in platelets count is called thrombocytopenia. • The increase in platelets count is called thrombocytosis. • Platelets are formed in bone marrow. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Functions of Platelets: 1. Role in blood clotting: • The platelets are responsible for the formation of intrinsic prothrombin activator. • This substance is responsible for the onset of blood clotting. 2. Role in clot retraction: • The cytoplasm of platelets contains the contractile proteins namely actin, myosin and thrombosthenin. • These contractile proteins are responsible for clot retraction. 3. Role in prevention of blood loss (Hemostasis): • It causes the constriction of blood vessels, seal the damaged part in blood vessels and play important role in plug formation. 4. Role in repair of ruptured blood vessels: • The platelets derived growth factor is useful for repair of ruptured blood vessels. 5. Role in defense mechanism: • The platelets kill foreign bodies by the process of phyagocytosis. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Plasma: • The plasma of the blood is formed by 92 to 93% of water and 7 to 8% of solids. • The solids are the organic and inorganic substances. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Organic substances presents in plasma: 1. Proteins: albumin, globulin, and fibrinogen. 2. Carbohydrates: Carbohydrates present are in the form of glucose. 3. Fats: Neutral fats, phospholipids and cholesterol. 4. Non-protein nitrogenous substances: Ammonia, amino acids, creatine, creatinine, Xanthin, hypoxanthine, urea and uric acid. 5. Internal secretions: The plasma contains many hormones. Enzymes: Amylase, alkaline phosphatase, acid phosphatase, lipase, esterase, proteases, and transaminase are present in plasma. Antibodies: The plasma contains many antibodies which are called immunoglobulins. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Inorganic substances present in plasma: • 1. Sodium, 2. Calcium, 3. Potassium 4. Magnesium 5. Chloride 6. Iodine 7. Iron 8. Phosphate 9. Copper Gases present in Plasma: • The respiratory gases oxygen and carbon dioxide are present in plasma. Functions of Blood: • 1. Nutrient function: • Nutritive substances like glucose, amino acids, Lipids and Vitamins derived from digested food are absorbed from gastrointestinal tract and carried by blood to different parts to the body, for growth and for production of energy. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
2. Respiratory function: • Transport of respiratory gases take place through the blood. • The oxygen is carried from alveoli of lungs to different tissues and Carbon dioxide is carried from tissues to alveoli. 3. Excretory function: • Waste products formed during various metabolic reactions in the tissues are removed by blood and carried to the excretory organs like kidney, skin, liver, etc. 4. Transport of hormones and enzymes: • The hormones and some of the enzymes are carried by blood to different parts of the body from the source of secretion. 5. Regulation of water balance: • Blood also regulates the water balance of the body. 6. Regulation of Acid-Base balance: • The plasma proteins and Hb act as buffers and help in regulation of acid base balance. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
7. Regulation of body temperature: • Because of the high specific heat of blood, it is responsible for maintaining the thermoregulatory mechanism in the body i.e. balance between heat loss and heat gain. 8. Storage function: • Blood serves as a source of water, proteins, glucose, sodium and potassium. • These substances are taken from blood during conditions like starvation, fluid loss, electrolyte loss, etc. 9. Defensive function: • Blood plays important role in the defense of the body. • The white blood cells are responsible for defense mechanism of the body. • Neutrophils and monocytes engulf the bacteria by phagocytosis. • Lymphocytosis are involved in immunity. • Eosinophils are responsible for detoxification, disintegration and removal of foreign proteins. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Coagulation of Blood: • Coagulation of blood is defined as the process in which the blood looses its fluidity and becomes a jelly like semisolid mass few minutes after it is shed out or collected in a container. • The semisolid mass formed after coagulation is called clot. • The clot is a mesh of thin fibrils entangling the blood cells. • These fibrils consist of fibrin threads. • The fibrin is formed from fibrinogen. • The substances necessary for clotting are called clotting factors. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Factor I (Fibrinogen): • Fibrinogen is a glycoprotein of molecular weight 340,000. • It consists of three pairs of non-identical polypeptide chains. • It is synthesized in liver and remains soluble in plasma. • During coagulation, it is converted into fibrin. Factor II (Prothrombin): • Prothrombin is a glycoprotein of molecular weight 70,000. • It is produced by liver and its synthesis requires vitamin K. • Human prothrombin has 9% carbohydrates including hexose, hexosamine and neuraminic acid. • In the presence of thromboplastin, it is converted into enzymatic thrombin which is having a molecular weight of about 34,000 daltons. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Factor III (Tissue Factor or Tissue Thromboplastin): • It is a lipoprotein complex. • It is obtained from tissues. • Purified preparations contain two fractions of M.W. 330,000 and 220,000. • Phospholipids greatly increase activity. • It converts prothrombin into thrombin in the presence of calcium ions. • Factor IV (Calcium ions): • This factor acts as a co-factor in coagulation. • It is essential for the formation of both extrinsic and intrinsic thromboplastin and also in the conversion of prothrombin into thrombin. • It is apparently involved in all three stages of clotting. • Removal of calcium or its binding in plasma prevents coagulation. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Factor V (Pro-accelerin or Labile Factor): • It is a plasma glycoprotein of molecular weight 290,000 (bovine). • It’s a heat protein synthesized in the liver. • This factor is necessary for the complete conversion of prothrombin into thrombin by intrinsic or extrinsic thromboplastin. Factor VI(Accelerin): • It is no longer used in coagulation theory and its number has not been reassigned. • This factor is a hypothetical activation product of pro-accelerin. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Factor VII (Pro-convertin or Stable Factor or Serum Prothrombin Accelerator): • It is a plasma protein having molecular weight 63,000. • It requires vitamin K for its synthesis. • It is synthesized in liver and is required in stage I of the extrinsic pathway. • It is associated with prothrombin. • It accelerates the formation of tissue thromboplastin from damaged tissues. • Factor VIII (Antihemophilic Factor or Antihemophilic Globin or Platelet cofactor-I): • It is a glycoprotein with a molecular weight of about 1.1 million. • It is synthesized in liver and is required for stage 1 of the intrinsic pathway. • Its deficiency causes hemophilia A. • It is closely associated with fibrinogen-that is why it disappears when the blood clots. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Factor IX (Christmas factor or Plasma Thromboplastin Component or Platelet Co-factor II): • It is a glycoprotein of molecular weight 55,400 (bovine). • It is synthesized in the liver and contains a single polypeptide chain. • Its formation requires vitamin K. • This factor is required for stage I of the intrinsic factor. • Deficiency causes the disorder called hemophilia B, a disease similar to hemophilia A. • The disease was first seen in a patient named Christmas, hence named as Christmas disease. Factor X (Stuart Factor or Stuart Power Factor): • Factor X is a glycoprotein of molecular weight of 55,000. • It is synthesized in the liver in the presence of vitamin K. • It is required for stage 1 and 2 of extrinsic and intrinsic pathways. • Deficiency results in nose bleeding into a joint or bleeding into soft tissues. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Factor XI (Plasma Thromboplastin Antecedent): • It is a glycoprotein of molecular weight 160,000. • It is synthesized by the liver. • It consists of two similar polypeptide chains. • It is required for stage I of intrinsic pathway. • Deficiency results into hemophilia C, a mild hemophilia of both males and females. • Factor XII (Hageman Factor or Surface Factor): • It is glycoprotein of molecular weight about 90,000. • It is activated on the surface of contact or by contact with glass and may assume a role in initiating coagulation outside the body. • It is required for stage 1 of the intrinsic pathway. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Factor XIII (fibrin Stabilizing Factor or fibrinase or Laki-Lorand Factor): • It is a glycoprotein of molecular weight 320,000. • Also isolated from platelets as a protein of molecular weight 150,000, it is required for stage 3 of clotting. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Blood Groups: • Blood groups are determined by the presence of antigen in RBC membrane. • When blood from two individuals in mixed, sometimes clumping (agglutination) of RBCs occur. • This clumping is because of the immunological reactions. • But, why clumping occurs in some cases and not in other cases was not known until the discovery of blood groups. • Austrian scientists Karl Landsteiner in 1901, made the discovery of existence of three blood groups in human beings. • He was honored with Nobel Prize in 1930 for this discovery. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
ABO blood groups: • Determination of ABO blood groups depend upon the immunological reaction between antigen and antibody. • Landsteiner found two antigens on the surface of RBCs. • He named them as antigen A and antigen B. • These antigens are also called agglutinogens because of their capacity to cause agglutination of RBCs. • He noticed corresponding antibodies or agglutinins in the plasma and named them anti A or α antibody and B or β antibody. • However a particular agglutinogen and the corresponding agglutinin cannot be present together. • If present it causes clumping of the blood. • Based on this, Landsteiner classified the blood groups. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Landsteiner’s Law: • Landsteiner’s law states that- • 1. If a particular antigen (agglutinogen) is present in the RBCs corresponding antibody (agglutinin) must be absent in the serum. • 2. If a particular antigen is absent in the RBCs the corresponding antibody must be present in the serum. • Based on the presence or absence of antigen A and antigen B blood is divided into four groups: • i) A group • ii) B group • iii) AB group • iv) O group Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
The antigens and antibodies present in different blood groups of ABO system are given in the following table. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Significance of blood groups: • The knowledge of blood group is essential for safe transfusion of blood. • In case of serious loss of blood due to injury or in various diseases like hemorrhage in lungs, stomach, loss of blood at the time of birth, extra uterine pregnancy and in serious form of anaemia the transfusion of blood is the only way by which the life can be saved. • 1. Medically it is important during blood transfusion and in tissue transplants. • 2. In society one should know his or her own blood group and become a member of the “Blood Doners” club so that he or she can be approached for blood donation during emergency conditions. • 3. Among the couples knowledge of blood groups helps to prevent the complications due to Rh incompatibility and save the child from the disorder like erythroblastosis foetalis. • 4. Judicially it is helpful in medicolegal cases to sort out parental disputes. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Other Blood Groups: • In addition to ABO blood groups and Rh factor many more blood group systems were found, however these systems of blood groups do not have much clinical importance. • 1. Lewis blood group: • This was first found in a lady named Mrs. Lewis. • In this lady the antibody found reacted with the antigens found on RBCs. • Presence of Lewis antigens in children sometimes leads to retarded growth and also cause transfusion reactions. • 2. MNS blood groups: • Theses blood groups are determined by their reactions with anti-M, anti-N and anti-S. • Theses blood groups rarely cause hemolysis after blood transfusion. • 3. Other blood groups are: • i) Auberger group ii) Bombay group iii)Lutheran group iv) Kell group v) Kidd group vi) Diego group vii) Duffy group viii) P group ix) I group x) Sulter X9 group Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Rh Factor: • Rh factor is an antigen (antigen D) present in RBC. • This antigen was discovered by Landsteiner and Wiener. • It was first discovered in Rhesus monkey and hence the name Rh factor. • This antigen has no naturally occurring antibody in monkey or man. • It is found that the blood of some persons contains Rh factor and others are without Rh factor. • Thus the persons whose RBC contain Rh factor are called Rh +ve persons and those without Rh factor are called Rh –ve persons. • Among Asian population 85% of people are Rh positive and 15% are Rh negative. • The percentage of Rh positive people is more among blacks. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Rh group system is different from ABO group system because, the antigen D does not have corresponding natural antibody (antibody D). • However, if Rh positive blood transfused to a negative person for the first time then anti D is formed in that person. • On the other hand there is no risk of complications if Rh positive person receives Rh negative blood. • Rhesus factor is an inherited dominant factor. • It may be homozygous Rhesus positive with DD or heterozygous Rhesus positive with Dd. • Rhesus negative occurs only with homozygous dd. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Clinical importance of Rh factor: • 1. Transfusion reactions due to Rh incompatibility: • The transfusion of Rh incompatible blood many times may produce serious conditions resulting in the death of the recipient. • When a Rh negative person receives Rh positive blood for the first time he is not affected much as there is no naturally occurring corresponding antibody. • But after one month the corresponding antibodies develop in the blood of recipient. • So when this person receives Rh positive blood for the second time there is reaction between donor RBCs and anti Rh formed in the recipients blood resulting in agglutination causing death of the recipient. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
2. Erythroblastosis foetalis: • The Rh factor sometimes becomes very important when parents belong to different Rh group. • Erythroblastosis foetalis is a disorder in foetus characterized by the presence of erythroblasts in blood. • When mother is Rh-ve and father Rh+ve, and she conceives a Rh+ve child then this first child is normal. • This is because the Rh antigen cannot pass from foetal blood into mothers blood through the placental barrier. • However, at the time of delivery, Rh antigen from foetal blood may leak into mothers blood because of placental detachment. • After first delivery the mother develops Rh antibody in her blood within a month. • When the mother conceives for the second time and the foetus happens to be Rh positive again the Rh antibody from mothers blood crosses placental barrier and enters the foetal blood and cause agglutination of foetal RBCs resulting in Haemolysis. • The Rh antigen can not cross the placental barrier whereas Rh antibody can cross it. • Haemolysis in the fetus causes jaundice. • To compensate Haemolysis there is rapid production of RBCs from bone marrow, spleen and liver also. • Because of this many large and immature cells in proerythroblastic stage are released into circulation. • Because of this the disease is called erythroblastosis fetalis. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Mechanism of Erythroblastosis fetalis Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Excessive Haemolysis result in anaemia, enlargement of liver and spleen, cardiac failure. • Severe jaundice cause brain damage in infants (Kernicterus). Prevention of erythroblastosis foetalis: • 1. A serum concentrate of anti Rh antibodies is injected into the mother soon after delivery (within 48 hours). The antibodies circulate in the maternal blood and destroy all the Rh positive factor before the antigen can initiate antibody response. • 2. Rh negative women should no be given transfusion of Rh positive blood at any time and certainly not before menopause. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Heart: Structure of human heart: • The heart is a hollow, conical organ, situated in the middle of the thoracic (chest) cavity slightly towards left side. • It is made up of cardiac muscles. • It is protected by rib cage and vertebral column. • It is about 12 cm in length and 9 cm in breadth. • It consist of four chambers-two auricles an two ventricles. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Pericardium: • Heart is enclosed in a double layered, transparent, thin sac called Pericardium. • The space between the inner and outer layers is called pericardial space. • It is filled with a fluid called pericardial fluid. • Pericardium and the pericardial fluid protect the heart from physical shocks or blows. Vena cavae or caval veins: • Very large veins that bring blood to the heart are called vena cavae or caval veins. Aortae: • Very large arteries that carry blood away from the heart are called aortae. Superior vena cava: • It is collects deoxygenated blood from the upper parts of the body. E.g, head and neck. Inferior Vena cava/post caval vein: • Brings deoxygenated blood from lower parts of the body. E.g., abdomen, hands and legs. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Pulmonary vein: • Which brings oxygenated blood from the lungs and opens into the left auricle. Coronary veins: • In addition to these major veins, a pair of veins called coronary veins bring deoxygenated blood from the walls of the heart. • These also open into right auricle. Systemic aorta: • Heart receives oxygenated blood from lungs and pumps it to various organs in the body through large aorta called systemic aorta. Pulmonary aorta: • Pulmonary aorta originates in the right ventricle. • Out side the heart, it divides into two branches-right and left pulmonary arteries which carry blood to right and left lungs. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Coronary arteries: • There is a pair of coronary arteries which carry oxygenated blood to the heart. • The left auricle receives oxygenated blood from the lungs by pulmonary veins. • The two auricles open in to the respective ventricles and the openings are guarded by auriculo-ventricular valves or AV-valves. • The right AV valves is called tricuspid valve(made of three flaps or cusps) while left AV valve is called bicuspid valve (made of two cusps) or mitral valve. Pace Maker: • Heart beat is regulated by the nodal tissue within the heart and sets of peripheral nerves from the brain. • The first such tissue is the sino-auricular node (S.A. node), located in the wall of the right auricle; near the superior vena cava. • This node has an inherent power of generating a wave of contraction known as pace-maker. • The other nodal tissue is the auriculo-ventricular node (A.V. node) which is located in the posterior right border of the inter-auricular septum, just above the ventricles. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
From the A.V. node arises a bundle of nerve fibres called bundle of His. • Within the myocardium of the ventricles the branches break up into a network of the branching fibres known as the fibres of Purkinje. • The impulses are transmitted by Purkinje fibres throughout the ventricular walls, causing the contraction of its muscles. • The muscles of both the ventricles contract simultaneously. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Cardiac Cycle: • Heart works as pumping station of circulatory system which circulates blood in the body. • The contraction of heart is called systole and its relaxation is called diastole. • Each heart beat therefore consists of systole and diastole. • Changes which occur in the heart during one beat are repeated in the same order in the next beat. • This cyclical repetition of various changes in heart from beat to beat is called cardiac cycle. • The heart beats 75 times per minute. • Therefore one cardiac cycle is completed within 0.8 second (60/75). This is called cardiac cycle time. • It means that every event in the cardiac cycle is repeated at an interval of 0.8 second. • In the cardiac cycle there are four main events auricular systole, auricular diastole, ventricular systole and ventricular diastole. • auricular systole= 0.1second, auricular diastole= 0.7 second. • ventricular systole= 0.3 Second, ventricular diastole = 0.5 second Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana
Control of working of heart: • 1. Nervous control: • The heart is abundantly supplied with parasympathetic (vagus nerve) and sympathetic nerve fibres. • In most vertebrates the heart is myogenic. • The impulse of contraction originates itself in the heart and the sympathetic nerve fibers supplying the heart can increase or decrease the cardiac activity while parasympathetic nerve fibres on the other hand inhibit the cardiac activity. • 2. Hormonal control: • The activity of the heart is also controlled by certain hormones. • The most important hormones which control the heart activity are: nor adrenaline and adrenaline. • These hormones increase and decrease the heart activity like sympathetic nerve fibres. • According to RINGER inorganic ions like calcium and potassium ions also control the activity of the heart. • High potassium ions follow a diastole arrest, while high calcium ions a systole arrest particularly in the frog heart. • pH is also a important factor which influences the heart activity. Mr. Shantaram Bhoye, Assistant Professor, Shri Pundlik Maharaj Mahavidyalaya, Nandura Rly., Dist. Buldana