Download
1 / 53
540 likes | 589 Views
Explore the high demands and various injuries in tennis players, from muscle tears to stress fractures. Learn about MRI's role in diagnosing and treating tennis-related injuries.

E N D
MRI EVALUATION OF TENNIS INJURIESTENNIS ELBOW AND BEYOND Peter P. Chow, M.D., M.P.H. Pacific Medical Imaging & Oncology Center, Alhambra, CA Valley Imaging Partnership, West Covina, CA
Tennis Injuries Overview • Extremely high demands on structural integrity of the body’s joints. • Repetitive, asymmetrical and technically challenging movements at high speed in dynamic settings. • Testing the limits of players’ physical and mental endurance
Tennis Injuries Facts-in ATP professional Players • 35-50% to lower extremities • 20% to upper limb • 20% to lower back • Chronic overuse conditions more likely to occur in upper body • Acute injuries more likely to occur in the lower limbs.
Muscle Injuries in Tennis Hamstring muscles Calf muscles
Middle-aged male pushing a stalled car and felt a pop in the calf
Rupture of Plantaris Tendon(Tennis Leg) • Middle-aged patients • Forced dorsiflection of the ankle with the knee in extention • Audible “pop” in the calf, with subsequent pain and swelling, and frequently with a palpable mass caused by hematoma • Often associated with ACL tear and posterolateral corner injuries
Calf Injury Tommy Haas
Medial Tibial Stress Syndrome • Also known as shin splints • Characterized by hyperintense signal along the anterior tibial border • Related to periosteal avulsion and periostitis at the medial soleus insertional site • Grade I (periosteal edema)thru grade IV (stress fracture)
BONE BRUISE-26 y/o M MR Tech 4 wk 7wk 9 wk after injury
Patellar tendinosis Jumper’s knee
Patellar Chondromalacia No. 1 USC player turned professional 30 y/o male, anterior knee pain
Hamstring Injury M. Sharapova at Pan Pacific Open, Feb. 2007
Hamstring Injuries • MR depicts the location and extent of injuries • MR useful in grading of muscular injuries: • Grade I – limited muscle fiber disruption • Grade II – partial tears at musculotendinous junction without retraction of muscle • Grade III – complete disruption of the musculotendinous junction, often with retraction • Treatment options depend on the location and severity of the injury
Melbourne, Australia 01/06 Kim Clijsters
The combined rotation and extension of the back during serving places high demands on the back
Pars Stress Fracture 30% of adolescents involved in sports will have an episode of low back pain. Lumbar spondylolysis is one of the causes of LBP in this age group of athletes. Athletes involved in sports requiring repetitive bending and straightening of the spine are most commonly affected Most patients have excellent clinical outcomes with conservative measures, and surgery is rarely necessary
Shoulder Pain in Athletes • AC joint sprain • Calcific rotator cuff tendinopathy • Clavicle fracture • Dislocated shoulder • Adhesive capsulitis • Rotator cuff tear • Subacromial bursitis
Shoulder Impingement Syndrome Adequate subacromial space Narrowed subacromial space
Articular sided partial tear High school varsity baseball pitcher-shoulder painbefore end of the season games
Extensor Carpi Ulnaris(ECU) Tendinitis • Related to racquet sports with repetitive wrist motion • Squash • Badminton • Raquetball • Tennis • Rowing • Tennis player with two-handed backhand using excessive ulnar deviation in nondominant wrist
Players who hit with a lot of topspin are at increased risk for extensor carpi ulnaris tendon injury
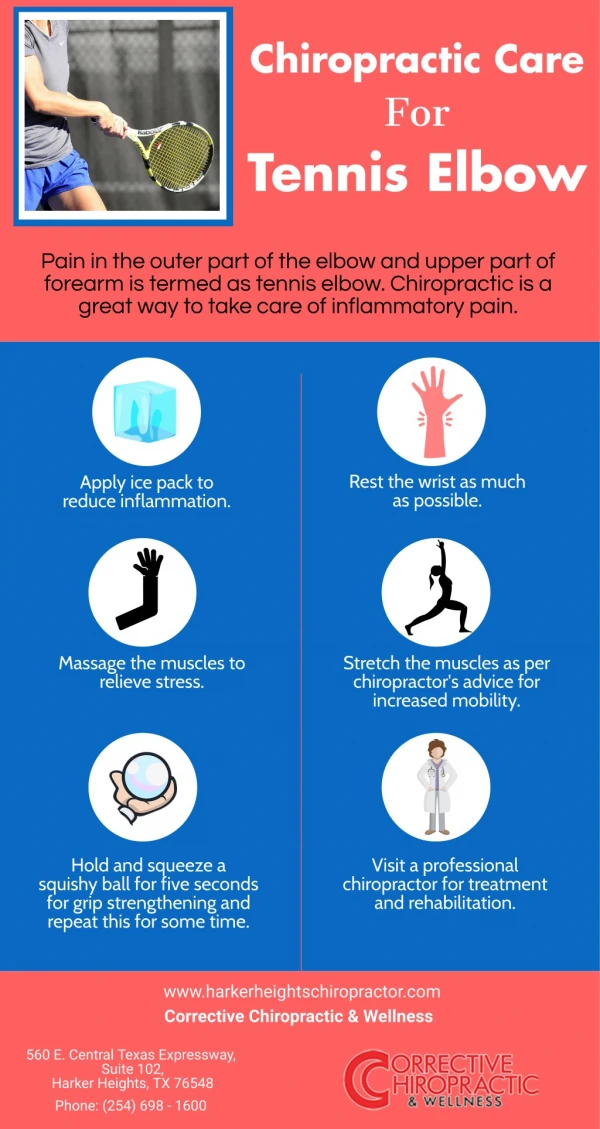
Tennis Elbow • Middle-aged female with a single-handed backhand who leads with elbow • Straightens elbow and extends wrist on contact • Placing the wrist extensors under excessive tension • Correct form – swinging from the shoulder with a straight arm and using the entire body to execute the stroke
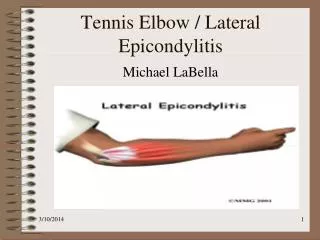
TENNIS ELBOW • A painful condition caused by inflammation or small tears of the wrist extensors and tendons, esp. extensor carpi radialis brevis rubbing over the lateral epicondyle and the radial head • Most experts believe that tennis elbow is caused by overloading of the forearm muscles due to faulty backhand technique
The backhandis generally found to be the prime cause of tennis elbow in non-professionalsdue to the complexity of this stroke. A bent elbow or "swinging" just at the elbow and not the entire arm, causes excess torques and forces in the elbow region. Other causes of tennis elbow are: Late backhand stroke with hyper-extended wrist. Too tight of grip. Excessive wrist "pop" on overhand serve. Forehand stroke with excessive wrist movement. Using too many “topspin” shots.
Electromyographic and cinematographic analysis of elbow function in tennis players using single- and double-handed backhand strokes It is generally believed that tennis players using a double-handed backhand rarely develop lateral epicondylitis since the helping arm appears to absorb more energy and changes the mechanics of the swing. Giangarra CE, et al, American Journal of Sports Medicine, Vol 21, Issue 3 394-399.