Download
1 / 39
440 likes | 652 Views
Agents That Affect Bone Mineral Homeostasis. Functions of the bone: Principal structural support for the body Ca and PO4 reservoir Space for hematopoesis. Two hormones serve as principal regulators of Ca & P homeostasis: parathyroid hormone (PTH) & vitamin D (active metabolite)

E N D
Agents That Affect Bone Mineral Homeostasis • Functions of the bone: • Principal structural support for the body • Ca and PO4 reservoir • Space for hematopoesis
Two hormones serve as principal regulators of Ca & P homeostasis: parathyroid hormone (PTH) & vitamin D (active metabolite) • Certain of secondary regulators— calcitonin, glucocorticoids & estrogens—are useful therapeutically
CLINICAL PHARMACOLOGY Conditions that alter bone mineral homeostasis: Effects on bone can result in: • osteoporosis (abnormal loss of bone; remaining bone histologically normal) • osteomalacia (abnormal bone formation due to inadequate mineralization) • osteitisfibrosa (excessive bone resorption with fibrotic replacement of resorption cavities)
HYPERCALCEMIA • Hypercalcemiacauses CNS depression, including coma, & is potentially lethal • Arrhythmia cardiovascular collapse give MgSO4 (IV) to offset the dynamic effect • Major causes (other than thiazide therapy) are hyperparathyroidism & cancer with or without bone metastases • Less common causes are hypervitaminosis D, sarcoidosis, thyrotoxicosis, milk-alkali syndrome - seldom require emergency ↓ of serum Ca (with exception of hypervitaminosis D) • Ca X PO4 must be < 55 mg2/dL2 in order to prevent ectopic calcification in soft vital tissues
Treatment of hypercalcemia 1. Saline Diuresis500-1000 mL/h of saline to reverse dehydration & restore urine flow + loop diuretic to ↑urine flow but also ↓Careabsorption in ascending limb of loop of Henle 2. If more prolonged treatment of hypercalcemia is required:1. BisphosphonatesEtidronate in saline IV for 3 days. Pamidronate appears to be more effective
Bisphosphonates • MOA: inhibit bone resorption • less than 10% of an oral dose of these drugs is absorbed. • Food reduces absorption even further empty stomach. • That’s why: pamidronate is not available as an oral preparation. • all currently available bisphosphonates have this complication (with the possible exception of etidronate) • Nearly half of the absorbed drug accumulates in bone; • C/I: Decreased renal function, esophageal motility disorders, and peptic ulcer disease are the main
3. Calcitonin: • ancillary treatment. • effect lasts for 6-10 hours. • Calcimar (salmon calcitonin) is available for parenteral & nasal administration (preferred) • MOA: (1) inhibits osteoclastic bone resorption ((although with time both resorption and firmation of bone are reduced) (2) In kidney: Reduces Ca and PO4 reabsorption • Useful for the treament of Paget’s disease, Hypercalcemia and osteoporossis
4. Gallium Nitrate (IV) • Acts by (-) bone resorption • Due to nephrotoxicity, patients should be well-hydrated & have good renal output before starting infusion
5. Plicamycin(Mithramycin):(risk of thrombocytopenia followed by hemorrhage), hepatic & renal toxicity 6. Phosphate: IV is hazardous procedure if not done properly: sudden hypocalcaemia, ectopic calcification, acute renal failure, hypotension • Must be given slowly (6-8 hrs) then switch to oral phosphate Very risky
7. Glucocorticoids: • Glucocorticoid hormones alter bone mineral homeostasis by: 1. antagonizing vitamin D-stimulated intestinal calcium transport, 2. by stimulating renal calcium excretion, and by 3. blocking bone formation • no clear role in acute treatment of hypercalcemia. • However, chronic hypercalcemia may respond within several days to glucocorticoid therapy • Prednisone (30-60 mg/day)
HYPOCALCEMIA • Main features (neuromsucular): tetany, paresthesias, laryngospasm, muscle cramps, & convulsions • Major causes in adult: hypoparathyroidism, vitamin D deficiency, chronic kidney disease & malabsorption, infusions of citrated blood • Neonatal hypocalcemia usually resolves without therapy • Treatment: Ca & vitamin D (or its metabolites)
Treatment of Hypocalcemia 1. Calcium: • IV: gluceptate, gluconate, chloride. Gluconate is the preferred form (less irritating to veins) • Rapid infusion can lead to cardiac arrhythmias • Oral: carbonate, lactate, phosphate, citrate Carbonate is preparation of choice: high % of Ca, ready availability, low cost, & antacid properties • Treatment: • Severe symptomatic hypocalcemia: slow infusion of 5-20 mL of 10% Cagluconate. Avoid rapid infusion (cardiac arrhythmias) • Less severe cases: oral Ca (carbonate to provide 400-1200mg of elemental Ca
2. Vitamin D 1,25(OH)2D3 (calcitriol), is the metabolite of choice for rapid action (↑serum Ca within 24-48 hrs). Also ↑ serum P but usually not observed early in treatment • Combined effects of calcitriol on both Ca & P make careful monitoring of serum Ca × P product important to avoid ectopic calcification
HYPERPHOSPHATEMIA • Causes: renal failure, hypoparathyroidism & vitamin D intoxication • Emergency treatment: by dialysis or glucose & insulin infusions • Chronic treatment: 1.↓ dietary phosphate 2. Ca supplements 3. Al(OH)3-containing antacids (potential to induce Al-associated bone disease) 4. Phosphate-binding gels (Sevelamer)
Diet Management of hyperphosphatemia • Minimize (but not avoid: cheese (no more than 1 oz per day, milk (250 mL per day), egg (no more than 1 per day- maximum 3-4 per week), heart, liver, kidney (no more than once per fortnight • Avoid: Pilchards, Sardines, Kippers, Herrings, Whitebait, Sprats, Fish Roe, Prawns or Crab, All Bran., Cocoa powder, Horlicks and Ovaltine, Evaporated milk, Chocolate (especially milk) and Fudge, Chocolate spread, Peanut butter, Nuts, popcorn.
Hypophosphatemia • Causes: e.g. hyperparathyroidism, vitamin D deficiency, idiopathic hypercalciuria, vitamin D-resistant rickets, various other forms of renal phosphate wasting • Leads to: • reduction in the intracellular levels of ATP, • interfere with normal hemoglobin-to-tissue oxygen transfer, and • Rhabdomyolysis • Treatment: Depending on the clinical situation, replacement options include dietary phosphate, oral phosphate preparations, and IV phosphate
SPECIFIC DISORDERS INVOLVING THE BONE MINERAL-REGULATING HORMONES
NUTRITIONAL VITAMIN D DEFFICIENCY • Vitamin D deficiency in pediatric & geriatric populations on vegetarian diets & with ↓sunlight exposure • Prevention: 800-1200 units/d of vitamin D • Treatment: higher dosages (4000 units/d) • 25(OH)D No other metabolite is indicated • Diet should also contain adequate amounts of Ca & P
CHRONIC RENAL FAILURE • Major problems: loss of 1,25(OH)2D & 24,25(OH)2D production, retention of P →↓ionized Ca levels → 2ry hyperparathyroidism • With loss of 1,25(OH)2D production, < Ca is absorbed from intestine & < bone is resorbed under influence of PTH → hypocalcemia→ exacerbation of hyperparathyroidism • Bones show mixture of osteomalacia & osteitisfibrosa • Less commonly hypercalcemia (adynamic bone disease)
Use of Vitamin D Preparations • Vitamin D in patients with substantial degree of renal failure cannot be converted to its active metabolites • Two analogs of calcitriol, doxercalciferol & paricalcitol, are approved for the treatment of 2ry hyperparathyroidism of chronic renal failure. They are less likely to induce hypercalcemia
Use of Vitamin D Preparations • 1,25(OH)2D3 (calcitriol) rapidly corrects hypocalcemia & at least partially reverses 2ry hyperparathyroidism & osteitisfibrosa. ↑ serum Ca in 1-2 days • Dihydrotachysterol, analog of 1,25(OH)2D, is equally effective. ↑Ca in 1-2 weeks • Neither calcitriol, nor dihydrotachysterol correct osteomalacia, & neither should be used in patients with hypercalcemia • Calcifediol (25[OH]D3) is < effective than calcitriol in stimulating intestinal calcium transport → < hypercalcemia • requires several weeks to restore normocalcemia
INTESTINAL OSTEODYSTROPHY • Malabsorption of Ca & vitamin D →combination of osteoporosis & osteomalacia • Liver disease may: • ↓production of 25(OH)D from vitamin D • Impaired secretion into bile of vitamin D metabolites & conjugates → deplete body of endogenous vitamin D & metabolites • In mild forms of malabsorption, vitamin D can be used. In severe disease: calcitriol & calcifediol
INTESTINAL OSTEODYSTROPHY • Malabsorption of Ca & vitamin D →combination of osteoporosis & osteomalacia • Liver disease may: • ↓production of 25(OH)D from vitamin D • Impaired secretion into bile of vitamin D metabolites & conjugates → deplete body of endogenous vitamin D & metabolites • In mild forms of malabsorption, vitamin D can be used. In severe disease: calcitriol & calcifediol
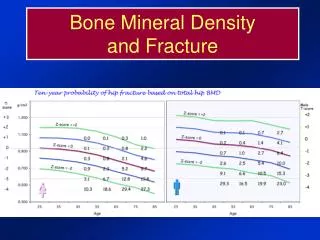
OSTEOPOROSIS • Osteoporosis is abnormal loss of bone predisposing to fractures. • Occurs in: • postmenopausal women • older men • Chronic/long term glucocorticoids therapy • hyperparathyroidism • malabsorption syndrome
Postmenopausal osteoporosis • may be accompanied by ↓1,25(OH)2D levels & ↓intestinal Ca transport • Estrogen deficiency → best treated with cyclic doses of estrogen • The most rapid loss of bone occurs within the first 5 years after menopause → administration of estrogens after this time may be < effective. • If estrogens are discontinued, accelerated bone loss may occur → treatment with estrogens should be started shortly after onset of menopause & may need to be continued for life
Risk of endometrial carcinoma is minimized by addition of a progestin • Estrogen therapy may be reserved for women with ↓bone mineral content at the time of menopause or those who lose bone rapidly in the first year after it • Treatment may reinitiate menstrual bleeding. • Other complications: hypertension & thrombophlebitis • Small ↑risk (if it exists at all) of breast cancer is outweighed by ↓ risk of osteoporosis
Vitamin D is often employed + dietary Ca supplementation • In several large studies, vitamin D supplementation (400-800 IU/d) has been shown to be useful • Calcitriol& its analog 1α(OH)D3↑bone mass & ↓ fractures • Use of these agents for osteoporosis is not FDA-approved, though they are used in other countries
Fluoride: the only agent that can directly (+) bone formation →↑ bone density • Calcitonin is approved for use in treatment of postmenopausal osteoporosis. Reduces bone resorption • Bisphosphonates: Alendronate & most recently, risedronate, are approved for treatment of osteoporosis • Raloxifene, SERM, without adverse effects on breast or uterus, has been approved for prevention (not treatment) of osteoporosis Like estrogen, ↑bone density & ↓fractures in spine. However, ↑risk of thrombophlebitis
PAGET'S DISEASE OF BONE • This is a disease of bone that initially results in the excessiveresorption of bone (by osteoclasts) followed by the replacement of normalbone marrow with vascular and fibrous tissue. • Manypatients are asymptomatic and diagnosed by routine X-rays. • The goal of treatment: ↓ bone pain & prevent progressive deformity, hearing loss, high-output cardiac failure, & immobilization hypercalcemia • Calcitonin & bisphosphonates are DOC • Treatment failures may respond to plicamycin (highly toxic)
Calcitonin is administered intranasally, SC or IM • Sodium etidronate, alendronate, risedronate, & tiludronate are bisphosphonates currently approved for this condition in the USA • Pamidronate is used in other countries • Etidronate, but not pamidronate & alendronate can cause osteomalacia & ↑incidence of fractures • Alendronate & newer bisphosphonates cause gastric irritation when used at high doses