Download
1 / 18
210 likes | 1.19k Views
Parenteral Nutrition. Dr Monidipa Banerjee Dr Papiya Khawas. Parenteral Vs Enteral Total vs Partial. Whom to give? . Can not feed - gut anomalies, GI surgery, NEC

E N D
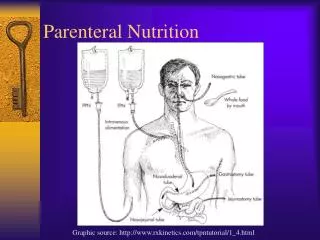
Parenteral Nutrition Dr Monidipa Banerjee Dr Papiya Khawas
Parenteral Vs Enteral Total vs Partial
Whom to give? • Can not feed - gut anomalies, GI surgery, NEC • Can not feed enough –Prematurity, renal disease, cardiac disease, growth failure of chronic disease • Should not feed – intestinal obstruction Inability to tolerate minimum 60 kcal/kg/d by enteral route
Whom not to give? • Metabolic acidosis • Acute renal failure – oliguria, ↑urea, ↑creat • Cholestatic jaundice
How to wean? • Oral feed to start as soon as baby is ready • Go up on oral feeds as tolerated • Keep total daily volume constant (TPN+ oral)
Infusion Routes • Umbilical vein- upto D7 • Long line – placed percutaneously - expensive • Broviac – placed surgically - expensive • Confirm proper line placement by x-ray • Peripheral vein can’t give higher conc.of dextrose,max12.5% problem with asepsis in prolonged TPN Ca, amino acid damages veins Used 80% of the time in our unit
Infrastructure • Place : OT, NICU, lamellar flow ( ideal ) • Prepared by: Doctor, trained nurse • Asepsis: person preparing should be fully scrubbed, using all new disposables every day • Delivery: syringe pump, infusion pump, High pressure infusion lines, chamber drip set,3 way connector/ BD connector • Monitoring: Trained nurse to monitor lines and baby
Protein:as crystalline amino acids Available: 6%&10% Aminoven, Primene. Each 100 ml of 10% Aminoven contains 10g of a.acid.(1ml contains 0.1g of a.acid) Calorie: 1g Protein = 4 kcal (prot:non-prot=1:6) Start:Can be started on Day 1 Dose: Starting with 0.5-1 g/kg/d, increment of 0.5g/kg/d, upto 3-3.5 g/kg/d. 1.5-2g/kg/d avoids catabolism Infusion:continuous over 24 hrs, mixed with dextrose Composition - 1
Lipid:emulsions with soybean oil preferred Available: 10%&20% Intralipid, Clipped. Each 100 ml contains 10g or 20g of lipid. (1ml contains 0.1g or .2g of lipid) Calorie: 1g Lipid = 9 kcal, 30%-40% of total calories Start:Usually started on Day 3 of TPN Dose: Starting with 0.5-1 g/kg/d, increment of 0.5g/kg/d, upto 3 g/kg/d. 0.5-1g/kg/d provides essential F.acids Infusion:continuous over 20-24 hrs, given separately Composition - 2
Carbohydrate:As dextrose, forms mainsubstrate (% tailored acc. to req. by combining 50% D & 5%D). Available: 5% Dext/IsoP - 5g/100ml = 50mg/ml 10% Dext -10g/100ml =100mg/ml 50% Dext -50g/100ml = 500mg/ml Calorie: 1g Carbohydrate= 4 kcal Dose:Starting 6mg/kg/min,↑10-12mg/kg/min Monitor: keep CBG 60-150 mg/dl Composition - 3
Composition - 4 • Multivitamins • Trace elements - usually added after 2 weeks of TPN • Heparin: if indicated ( e.g. UVC, centrallines)0.5-1 unit heparin/ml of TPN
Normal daily requirement Na+ 2-4 mmol/kg/d add >48 hrs K+ 2 mmol/kg/d add >48 hrs & normal urinary flow Ca++ 1 mmol/kg/d or add Day 1 2 mEq/kg/d or 75mg/kg/d Mg++ 0.3mEq/kg/d (0.25 ml/kg/d of 50% MgSO4 –maintenance dose) PO4 isolated P preparation not available Electrolytes
How much? • Total fluid req. >day 5 = 150-180ml/kg/d • Volume for TPN= total fluid – other infusions • Volume for TPN = Lipid + AA + Dext + Electrolytes + MVI • Total calorie req. = ~ 100 kcal/kg/d • Calories from Non-protein:Protein source maintained at a ratio above 6:1 to prevent catabolism.
Parenteral nutrition Intralipid (separately by syringe pump via a 3-way connector) Aminoven + Isolyte-P/ 5% Dextrose 50% Dextrose + MVI + Heparin (0.5 - 1unit/ml) + Add. electrolytes, as reqd.
Remember!!! • Strict asepsis • 24-hr TPN prepared at a time • Changing infusion sets daily (ideal) • New amino acid, lipid bottles daily (ideal) • Separate IV access for other drugs • Serum Na, K on alt. days; urea, creatinie,Ca biweekly; P, Mg, LFT, triglycerides weekly (ideal)
Complications • Mechanical: thrombosis, embolism, skin slough • Infectious: particularly staph epidermidis, candida • Metabolic: hypoglycaemia, hyperglycaemia, cholestasis