Download
1 / 40
400 likes | 413 Views
Stages of Maternal-Offspring interactions Conception, menstruation and early survival of the embryo Invasion of the placenta Maternal-fetal food fights (a) Glucose concentration (b) Blood supply Gestation length Survival of the fattest and cutest Sucking, crying, whining, weaning

E N D
Stages of Maternal-Offspring interactions • Conception, menstruation and early survival of the embryo • Invasion of the placenta • Maternal-fetal food fights (a) Glucose concentration (b) Blood supply • Gestation length • Survival of the fattest and cutest • Sucking, crying, whining, weaning • Survival and increased reproduction of the slower-developing child
Maternal-fetal interactions over resources during gestation replaced by maternal-child interactions over resources during lactation period Gestational interactions are biochemical After birth, interactions are also behavioral; suckling and crying can be seen as forms of begging behavior PLACENTA->BREAST In public health literature, interests of mother and young child are seen as fully coincident Main health concerns in gestation: fertility, miscarriage, growth restriction, pre-eclampsia, gestational diabetes Main health concerns in lactation period: failure to thrive, infant obesity, colic: difficulty in establishing postnatal nutrition is one of main reasons that new mothers visit family doctor
SUCKLING: KEY CONSIDERATIONS (JK Wells, 2002) The lactational infant growth period is the only time after birth when growth is regulated (and limited) by food intake - later, it is regulated hormonally Early growth is an important determinant of survival in childhood and adult size, which is positively associated with fitness Suckling, especially at night and especially in nutritionally-stressed mothers, causes lactational amenorrhea (natural contraception, due to high prolactin) Suckling itself is not energetically expensive for children, but for mothers it is much more expensive than gestation (up to 30% of daily energy, vs 10% for gestation). Costs of lactation are alleviated via maternal fat stores and complementary foods Mothers put benzodiazepine-like sedatives in breast milk, which suggests a strategy of mothers to constrain suckling Optimal time of weaning for mother is earlier than optimal time for child; in some primates, intense suckling near weaning, but mother withholds nipple more -> weaning conflict, also found in humans
Mother controls: Infant controls: -access to nipple -crying frequency,intensity -content of breast milk -attempted suckling -lactational amenorrhea system -suckling intensity, duration -threshold of response to crying
INFANT CRYING: KEY CONSIDERATIONS (JK Wells, 2002) Crying is energetically costly (metabolic rate 20x higher than in quiet sleep, and it is a ‘graded signal’ (continuously adjustable) (2) Crying occurs in context of hunger, pain, fear, vocalization and language, and separation - mainly separation in non-human primates, mainly hunger in humans (3) Crying and intake peak during highest-growth stage (~6 weeks) Six weeks: 40% of energy intake to growth Three months: 30% Six months: 10% One year: 5% (4) Crying thus appears to usually serve as a (costly) more-or-less honest signal of need (5) Crying may also serve as a signal of infant vigor, quality, to some degree (6) Near weaning, crying shifts to become more nocturnal FUNCTIONAL DESIGN
Genetic and epigenetic evidence for mother-offspring conflict over suckling Mouse knockouts of several paternally-expressed imprinted genes (PEG3, GNASxl) exhibit severely-impaired suckling behavior, due to hypothalamic and orofacial muscle defects (2) In humans, Silver-Russell syndrome (due to biases towards maternal-gene expression) involves impaired orofacial muscle development that interferes with suckling and other feeding In humans, Angelman syndrome involves increased suckling attempts, Prader-Willi syndrome involves decreased suckling attempts
Angelman: maternal deletion of 15q11-q13; or paternal UPD15; or UBE3A mutation Oppositely-imprinted neurogenomic disorders: Prader-Willi & Angelmansyndromes • Prader-Willi: paternal deletion of 15q11-q13; or maternal UPD15
prolonged suckling frequent crying hyper-active/sleepless ‘picky’ about food after weaning in many cases AngelmanPrader-Willi • poor suckling • weak crying • inactive/sleepy • after weaning, develop hyperphagia, forage on own unselectively
INFANT CRYING: A SIMPLE VERBAL MODEL (JK Wells, 2002) -Initially, crying signals need -When provisioning is generous, needs inflate into wants -When provisioning is poor, crying level should reduce, to conserve energy -Maternal and offspring strategies are assumed to have evolved under resource limitation and no artificial contraception - infant is selected in context of sibling competition, mother in context of optimal investment in multiple offspring -Recent changes, resulting in mismatches between ancestral and current environments High resource levels in developed and some developing countries, may alter behavior of infant (2) Altered social environment, may alter maternal receptivity to signalling, or interpretation of signal
Maternal response threshold (responsiveness to given level of crying; persistence in fostering suckling Offspring demand (levels of crying, attempted suckling) Dynamically-balanced ‘tug of war’ Usual situation,as in gestation
Maternal response threshold (responsiveness to given level of crying; persistence in fostering suckling Offspring demand (levels of crying, attempted suckling) Dynamically-balanced tug of war OR Demand high and/or response threshold low OR Demand low and/or response threshold high Usual situation,as in gestation Overnutrition Undernutrition
Implications of mismatches for health and disease, in context of mother-infant confluence and conflict of interest Overnutrition and early-onset obesity -medical criteria is centiles of weight adjusted for length -evolutionary criteria is offspring gaining more resources than optimal for mother to give, to point of maladaptation for both Increased transfer of resources to offspring predicted under: increased offspring demand intensity: TRUE, when resources are abundant fitness cost of signaling is lower; mothers also give food and drink to resolve distress -> crying develops into ‘blackmail’ (b) lower threshold of response: TRUE, changes in parental attitudes, style (c) cost of resource decreases: TRUE, energy is no longer limiting, energetic tradeoffs are absent Also, (d) formula now has a higher energy density than breast milk, and with formula intake is not constrained by maternal production
Implications of mismatches for health and disease, in context of mother-infant confluence and conflict of interest (2) Undernutrition and failure to thrive -medical criteria is centiles of weight adjusted for length -evolutionary criteria is offspring gaining less resources than optimal for mother or child Decreased successful food transfer to child, due to some combination of reduced demand by child, increased response threshold by mother -Found in some neurodevelopmental disorders (Prader-Willi, Silver-Russell) but these are rare -Appears commonly due to subtle oral-motor dysfunction in child, and/or psycho-social factors in mother -Low levels of demand (crying, soliciting suck) can jeopardize milk supply -Weak suckling also reduces efficiency of bottle-feeding -Signaling (crying) by baby develops to be cost-ineffective (as in famine) -Parents may not recognize feeding difficulties, lack reference information -Hospitalization does not address root cause - behavioral intervention more effective
Maternal response threshold (responsiveness to given level of crying; persistence in fostering suckling Offspring demand (levels of crying, attempted suckling) Dynamically-balanced tug of war OR Demand high and/or response threshold low OR Demand low and/or response threshold high Usual situation,as in gestation Overnutrition Undernutrition
Implications of mismatches for health and disease, in context of mother-infant confluence and conflict of interest (3) COLIC - ‘excess’, inconsolable crying of unknown cause Often attributed to gastrointestinal pain, but no good evidence for this May be associated with crying as a signal of infant health and vigor, when such crying is energetically-affordable -> colicky infants do not show reduced growth, but otherwise few tests, little evidence May be started or exacerbated by initial misinterpretation of signaling (is evidence for maternal-infant behavioral disruptions with colic)
-Maternal response threshold (responsiveness to given level of crying; persistence in fostering suckling Maternal-offspring communication dysregulated -Offspring demand (levels of crying, attempted suckling) Offspring demand, vigor signals dysregulated, high Dynamically-balanced tug of war OR Demand high and/or response threshold low OR Demand low and/or response threshold high OR Demand, vigor high, response threshold high or dysregulated Usual situation,as in gestation Overnutrition Undernutrition COLIC
CONCLUSIONS: INFANT CRYING, FEEDING, LACTATION (1) Problems with infant feeding seen as physiological may be mainly behavioral, and are usefully understood in terms of evolved mother-offspring interactions involving mix of cooperation of conflict, and mismatches to ancestral environments (2) There is a direct and close analogy between feeding during gestation, and feeding during lactation, in that both apparently involve evolved ‘tugs-of-war’ between mother and offspring (3) Disruption in these tugs-of-war can help explain some of the major public health problems associated with infant feeding (4) Further tests based on functional design and the comparative method are urgently needed
Sucking, crying, whining, WEANING WEANING: KEY CONSIDERATIONS Defined as beginning of food supplemental to breast-feeding, ending with cessation of breastfeeding Humans wean their children considerably earlier in the life course (3 years) than do other apes (5-7 years); the age of weaning is highly variable within and between cultures; humans are only primate that weans offspring before they can forage independently; interbirth intervals are very short in humans, for primates; huge effects on human demography. Figure-> Weaning marks a shift to allo-caregiver support (not independence) (4) Period just after weaning (usually due to birth of sibling) involves spike in mortality of weaned child, in traditional societies; interbirth interval and child mortality are highly correlated in traditional societies (5) Appropriate weaning practices have huge effects on human health and well-being in developed and developing countries
Nutrition-related life-history stages for a generalized mammal
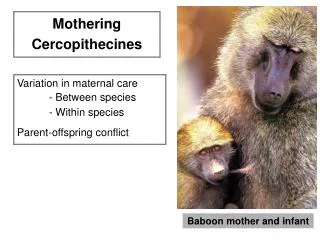
Evolution of human child feeding compared to other mammals, primates
Transitional & flexible complementary feeding appear unique to humans
Current international recommendations for optimal growth and development of healthy humans in favorable environment (1) start breastfeeding within one hour of birth (2) exclusive breast-feeding for six months, followed by nutrient-dense pathogen-free foods (3) gradual introduction of high-quality ‘family food’, with continued breast-feeding into the third year In reality, young child feeding practices are clinically suboptimal for most children and their mothers Why? A few reasons for the mismatch: Infant formula availability (overnutrition, no immunological or other trace-nutrient components), loss of extended-family support, economically-curtailed breastfeeding, dysregulation of mother-offspring conflicts
Good Bad
ROLE OF MOTHER-OFFSPRING CONFLICT IN WEANING Time course of parent-offspring conflict over parental investment Both benefit Child benefits Both suffer costs Costs on mother As child ages and grows, benefits of breast-feeding to child and mother decline, and costs to mother increase, in terms of her investment in other offspring Mother prefers to wean child earlier than child prefers to be weaned
Supports and constraints (trade-offs) on breast-feeding vary among human cultures
The balance of supports and constraints influences when supplemental foods are introduced
One example of how the conflict plays out, with early supplementation
When supplementation occurs before conflict period, both mother and child suffer reduced fitness, from high infant morbidity and mortality
Who controls the timing, duration of weaning, and how? Mothers control access to the breast and supplementary food presentation, subject to tradeoffs and constraints Offspring control their behaviour: tantrums, whining, and persistence over breastfeeding and acceptance of supplementary foods, or regression (acting younger than actual age) - ‘psychological warfare’ (Trivers 1972) Mothers hold the balance of power regarding cessation of breastfeeding, and introduction of supplementary foods
Prader-Willi syndrome and the evolution of human childhood (Haig and Wharton 2003) -before usual age of weaning (2 or 3) weak muscle tone, poor suckling, weak crying -after weaning, develop hyperphagia, forage on own, highly unselectively May reflect historical genomic conflict over nature and timing of child feeding -> Prader-Willi baby is ‘ideal’ in terms of low energetic costs imposed on mother
Stages of Maternal-Offspring interactions • Conception, menstruation and early survival of the embryo • Invasion of the placenta • Maternal-fetal food fights (a) Glucose concentration (b) Blood supply • Gestation length • Survival of the fattest and cutest • Sucking, crying, weaning, whining • Human childhood growth: survival and increased reproduction of the slower-developing child
KEY CONSIDERATIONS: Human growth patterns, compared to other primates Humans evolved from (precocial) primates, but have evolved to be altricial (relatively helpless and dependent, physically) (2) Human grow very quickly in the first year, especially in brain size (maintain high fetal rate); infant growth is nutrient-regulated - reduce vulnerable period (3) Humans grow very slowly between age 2 and puberty; childhood growth is hormonally-regulated - they are staying young ‘on purpose’, with a big brain.Then comes the adolescent growth spurt (4) Long, extended lifespan, with slow aging (5) Menopause
Why do human children develop so slowly, physically, from weaning until reproductive maturity? Selective advantage from increased parental investment, in competitive environment (2) Key role of brain development and maturation in childhood - development of language & motor skills, gaining cultural knowledge (3) Extrinsic mortality is low after infancy and weaning, so it is relatively ‘safe’ to develop slowly (costs are low) MISMATCH: Secular trend towards earlier age of menarche in girls due to recent enhanced nutrition (especially fat), results in shortening of childhood stage, asynchrony of brain & body development
Stages of human life history Gestation Childhood (3) Reproductive period (4) Post-reproductive period GROWTH, MAINTENANCE AND REPRODUCTION ARE SUBJECT TO TRADE-OFFS TO ANALYZE SUCH TRADE-OFFS, WE USE LIFE-HISTORY THEORY GROWTH and maintenance REPRODUCTION and maintenance MAINTENANCE and allo- parental care