Download
1 / 1

E N D
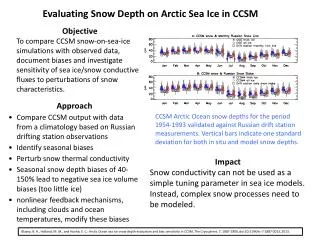
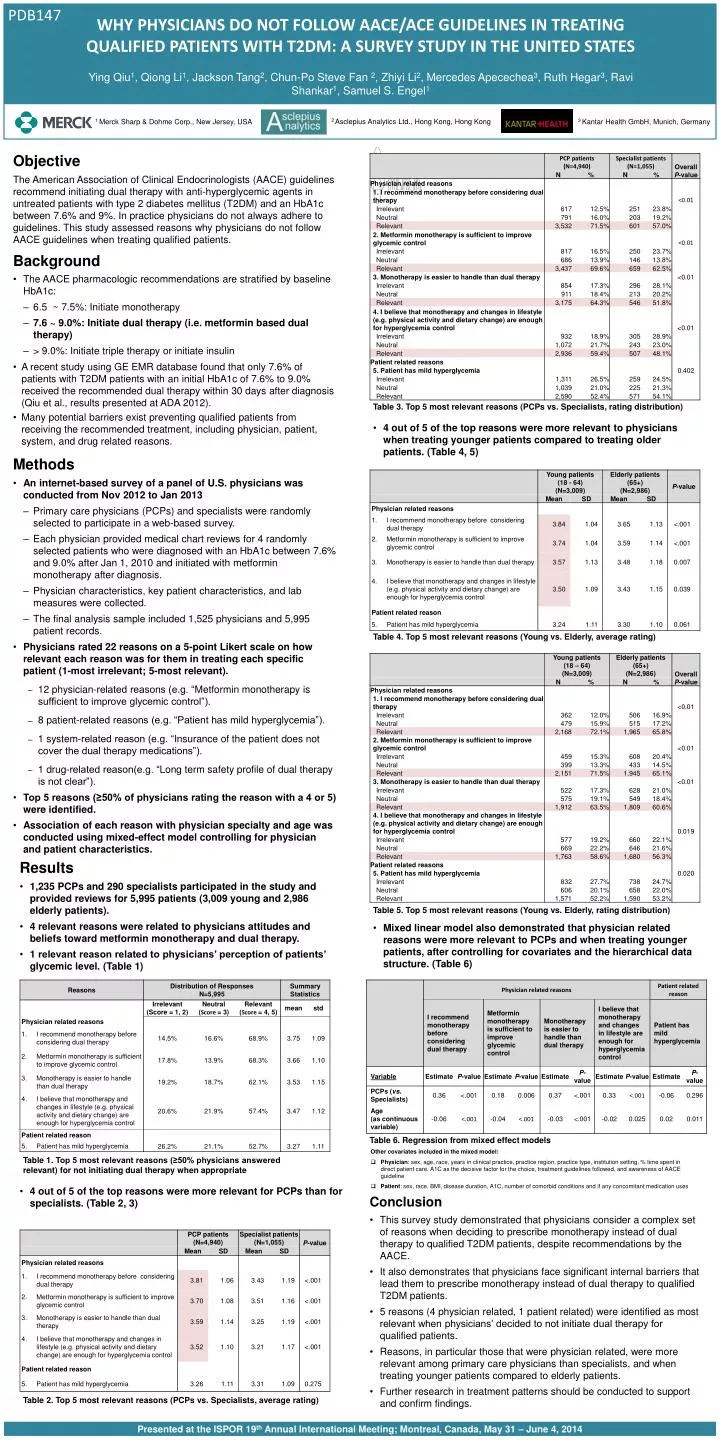
Objective • The American Association of Clinical Endocrinologists (AACE) guidelines recommend initiating dual therapy with anti-hyperglycemic agents in untreated patients with type 2 diabetes mellitus (T2DM) and an HbA1c between 7.6% and 9%. In practice physicians do not always adhere to guidelines. This study assessed reasons why physicians do not follow AACE guidelines when treating qualified patients. • Background • The AACEpharmacologic recommendations are stratified by baseline HbA1c: • 6.5 ~ 7.5%: Initiate monotherapy • 7.6 ~ 9.0%: Initiate dual therapy(i.e. metformin based dual therapy) • > 9.0%: Initiate triple therapy or initiate insulin • A recent study using GE EMR database found that only 7.6% of patients with T2DM patients with an initial HbA1c of 7.6% to 9.0% received the recommended dual therapy within 30 days after diagnosis (Qiu et al., results presented at ADA 2012). • Many potential barriers exist preventing qualified patients from receiving the recommended treatment, including physician, patient, system, and drug related reasons. Table 3. Top 5 most relevant reasons (PCPs vs. Specialists, rating distribution) • 4 out of 5 of the top reasons were more relevant to physicians when treating younger patients compared to treating older patients. (Table 4, 5) • Methods • An internet-based survey of a panel of U.S. physicians was conducted from Nov 2012 to Jan 2013 • Primary care physicians (PCPs) and specialists were randomly selected to participate in a web-based survey. • Each physician provided medical chart reviews for 4 randomly selected patients who were diagnosed with an HbA1c between 7.6% and 9.0% after Jan 1, 2010 and initiated with metformin monotherapy after diagnosis. • Physician characteristics, key patient characteristics, and lab measures were collected. • The final analysis sample included 1,525 physicians and 5,995 patient records. • Physicians rated 22 reasons on a 5-point Likert scale on how relevant each reason was for them in treating each specific patient (1-most irrelevant; 5-most relevant). • 12 physician-related reasons (e.g. “Metformin monotherapy is sufficient to improve glycemic control”). • 8 patient-related reasons (e.g. “Patient has mild hyperglycemia”). • 1 system-related reason (e.g. “Insurance of the patient does not cover the dual therapy medications”). • 1 drug-related reason(e.g. “Long term safety profile of dual therapy is not clear”). • Top 5 reasons (≥50% of physicians rating the reason with a 4 or 5) were identified. • Association of each reason with physician specialty and age was conducted using mixed-effect model controlling for physician and patient characteristics. Table 4. Top 5 most relevant reasons (Young vs. Elderly, average rating) • Results • 1,235 PCPs and 290 specialists participated in the study and provided reviews for 5,995 patients (3,009 young and 2,986 elderly patients). • 4 relevant reasons were related to physicians attitudes and beliefs toward metformin monotherapy and dual therapy. • 1 relevant reason related to physicians’ perception of patients’ glycemic level. (Table 1) Table 5. Top 5 most relevant reasons (Young vs. Elderly, rating distribution) • Mixed linear model also demonstrated that physician related reasons were more relevant to PCPs and when treating younger patients, after controlling for covariates and the hierarchical data structure. (Table 6) Table 6. Regression from mixed effect models • Other covariates included in the mixed model: • Physician: sex, age, race, years in clinical practice, practice region, practice type, institution setting, % time spent in direct patient care, A1C as the decisive factor for the choice, treatment guidelines followed, and awareness of AACE guideline • Patient: sex, race, BMI, disease duration, A1C, number of comorbid conditions and if any concomitant medication uses Table 1. Top 5 most relevant reasons (≥50% physicians answered relevant) for not initiating dual therapy when appropriate • 4 out of 5 of the top reasons were more relevant for PCPs than for specialists. (Table 2, 3) • Conclusion • This survey study demonstrated that physicians consider a complex set of reasons when deciding to prescribe monotherapy instead of dual therapy to qualified T2DM patients, despite recommendations by the AACE. • It also demonstrates that physicians face significant internal barriers that lead them to prescribe monotherapy instead of dual therapy to qualified T2DM patients. • 5 reasons (4 physician related, 1 patient related) were identified as most relevant when physicians’ decided to not initiate dual therapy for qualified patients. • Reasons, in particular those that were physician related, were more relevant among primary care physicians than specialists, and when treating younger patients compared to elderly patients. • Further research in treatment patterns should be conducted to support and confirm findings. Table 2. Top 5 most relevant reasons (PCPs vs. Specialists, average rating)