Download
1 / 31
320 likes | 435 Views
Cerebral Palsy (CP). Disorders characterized by early onset and impaired movement and posture. It is a non-progressive disease. Incidence. 1.9-2.3 in every 1000 live births in prevalence since the 1960’s due largely to the improved survival of VLBW infants. Etiology.

E N D
Cerebral Palsy (CP) Disorders characterized by early onset and impaired movement and posture. It is a non-progressive disease.
Incidence • 1.9-2.3 in every 1000 live births • in prevalence since the 1960’s due largely to the improved survival of VLBW infants.
Etiology • Greatest prevalence is seen in prematurely delivered infants. • Formerly thought to be R/T perinatal birth asphyxia, but now it is known that CP more commonly results from existing prenatal brain abnormalities. • 24% of cases have no identifiable cause.
Pathophysiology • Difficult to determine exactly • ANOXIA is most significant factor to cause pathologic brain damage. This is often 2ndary to other etiology. • The area of the lesion in the brain mostly determines the subsequent pathology.
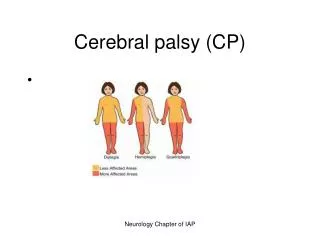
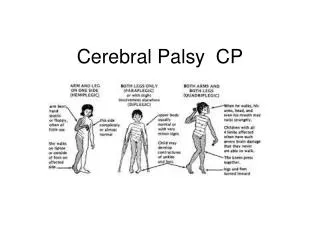
Clinical Classification of CP(see box 40-2 in Wong, p.1693 9th ed.)
Clinical Manifestations ( Box 40-4, Wong, p. 1695 9th ed.—Possible Signs) • Delayed gross motor development—universal manifestation of CP • Especially significant if other developmental behaviors e.g. speech & personal social are normal • Abnormal motor performance—Early sign is preferential unilateral hand use that may be apparent at ~6months of age.May stand or walk on toes
Clinical Manifestations (Box 40-4, Wong, p. 1695 9th ed. —Possible signs) • Alterations of Muscle Tone— • or resistance to passive movements is a sign of abnormal muscle tone. • Child may exhibit opisthotonic postures and stiffness on handling, dressing, or diapering. • Abnormal Postures— • From an early age, a child lying in a prone position will maintain the hips higher than the trunk with the legs and arms flexed or drawn under the body. • Spasticity may be mild or severe.
Clinical Manifestations (Box 40-4, Wong, p. 1695 9th ed. —Possible signs) • Reflex abnormalities— • Persistence of primitive infantile reflexes is one of the earliest clues to CP. • Associated Disabilities and problems— • Intellectual impairment—possible, but 70% are WNL • ADHD—poor attention span, marked distractibility, hyperactive behavior,and defects of integration • Seizures—most common in postnatal acquired hemiplegia • Drooling, feeding and speech needs, risk of aspiration & possible inadequate gas exchange. • Orthopedic complications • Constipation • Dental caries, malocclusion, gingivitis • Nystagmus, amblyopia & hearing loss
Diagnostic Evaluation • Neurologic Examination & History are the primary modalities for diagnosis • Recognizing etiologic factors that put the infant at risk is critical in the assessment and diagnostic process.
Therapeutic Management: General Concepts Box 40-5 p. 1696 9th ed.Therapeutic Interventions for CP • Broad aims: • Establish locomotion, communication, and self-help • Gain optimum appearance & integration of motor functions • Correct associated defects as effectively as possible • Provide educational opportunities adapted to the needs and capabilities of the individual child • Promote socialization experiences with other affected and unaffected children.
What is done— • Mobilizing devices—braces, crutches, wheelchairs, walkers • Surgery—when spasticity causes further deformities • Medication—drugs to spasticity are often NOT helpful in CP. Antianxiety meds may help child with athetosis.Skeletal muscle relaxants e.g. baclofen, methocarbamol (Robaxim), or dantrolene (Dantrium) & Valium may help short-term for older children & adolescents. Antiepileptic meds, e.g. phenobarbital & phenytoin are used routinely for children with seizures & CP.
What is done—(cont-d) • Technical aids—e.g. electromechanical toys that use biofeedback; microcomputers combined with voice synthesizers, or activated with a head-stick, tongue,or other voluntary muscle movement over which the child has control. • Other Considerations—care of vision & hearing deficits as well as dental care is essential early on.
Therapeutic Management: Therapies, Education, Recreation • Physical Therapy—one of the most commonly used conservative txmodalites. Involves PT, family, and nsg • Functional & Adaptive Training (Occupational Therapy)—training in manual skills and ADL’s must be started early • Speech Therapy—start early to prevent speech problems. • Education—individualize to the needs of the child • Recreation—sports, physical fitness, & recreation programs are encouraged for children with CP
Nursing Care (see Care Plan pp.1702-1703 in 9th ed.) • Reinforce therapeutic plan/assist in Normalization • Address Health Maintenance needs • Watch for fatigue, nutritional needs, safety needs • Support family • Help them cope with the emotional aspects of the disorder • Make appropriate referrals to support groups e.g United Cerebral Palsy Association. http://www.ucpa.org/search.cfm • Support hospitalized child— • the nurse’s actions should convey acceptance, affection, and friendliness and promote a feeling of trust and dependability.
Muscular Dystrophy Gradual degeneration occurs in muscle fibers progressive weakness and symmetric wasting away of skeletal muscle
3 Types of DystrophyTable 40-2; p. 1725 9th ed. • Pseudohypertophic (Duchenne) • X-linked Recessive • 1-3 years of age • Lordosis, Waddling gait • Rapid progression— • Death 15-25 after onset • Website Part 1 with newest Guidelines from MDA—12/09 • Website Part 2 with newest multidisciplinary guidelines from MDA—12-09
Limb-Girdle • Onset after 8 y/o • Weakness of proximal muscles of pelvic and shoulder girdle • Slow progression • Incapacitated 20 years after onset • OR slight disability
Facioscapulohumeral(Lansouzy-Dejerine) • Early adolescence • Symptoms • Lack of facial mobility • Can’t raise arms over head • Shoulders slope forward • VERY SLOW PROGRESSION
General Dx Tests • Serum Creatinine Phosphokinase (CPK) • Electromyography (EMG) • Muscle Biopsy
General Trx • Supportive • Physical Therapy • Orthopedic Trx (casting, bracing, surgery) to minimize deformities and maintain ability to perform ADL’s
Duchenne • Most severe + most common type • X-linked recessive • Inherited MOTHER carrier/Son Symptoms • Genetic mutation—ABSENT skeletal muscle protein
S/S • Muscle weakness by 3 y/o • Hx delayed motor development • Abnormal Gait, Waddling • Falls Frequently • Marked Lordosis when standing • Gower’s Sign
S/S • Enlarged calves, upper arms, thighs fatty infiltration of muscle pseudohypertrophic • Contractures • 12 y/o = unable to walk • Weakened respiratory muscles • Death
Complications • Contracture Deformities • Atrophy • Trx • PROM & AROM • Casting/Bracing • Rigid Corset • Frequent Rest • PT 3 hrs of ambulaton/day
Complications • Infections d/t decreased vital capacity and atrophy of resp muscles • Obesity d/t overfeeding and decreased activity • Antibiotics • Resp. Trx • Chest Physiotherapy • Diet • Recreation as tol. • Maintain mobility as long as possible
Cardiac Complications • D/T Weakening of Cardiac Muscle • Treatment • Digoxin • Diuretics e.g furosemide
Diagnosis • Serum Enzymes • Creatinine Phosphokinase • Aldoase • Glutamic-oxaloacetic transaminase (SGOT) • Very high levels in 1st 2 years of life • Levels decrease as muscle deteriorates • WNL when severe wasting and disability
Diagnosis • Muscle Biopsy • Degeneration of muscle fibers • Fatty deposits • Fibrosis • EMG • Diminished duration and amplitude of existing motor unit potentials
Nursing Care • Help maintain independence • Continual evaluation of capabilities • Home Assessment • Set-up w/c assessible?, wide doors?, etc • Buying clothes • Respite Care • Family Involvement • Genetic Counseling