Download
1 / 1
10 likes | 99 Views
Stigmatization as a Pathway to Disrupted Self-Development in Sexually Abused Youth Candice Feiring, The College of New Jersey Charles Cleland, National Development & Research Institutes.

E N D
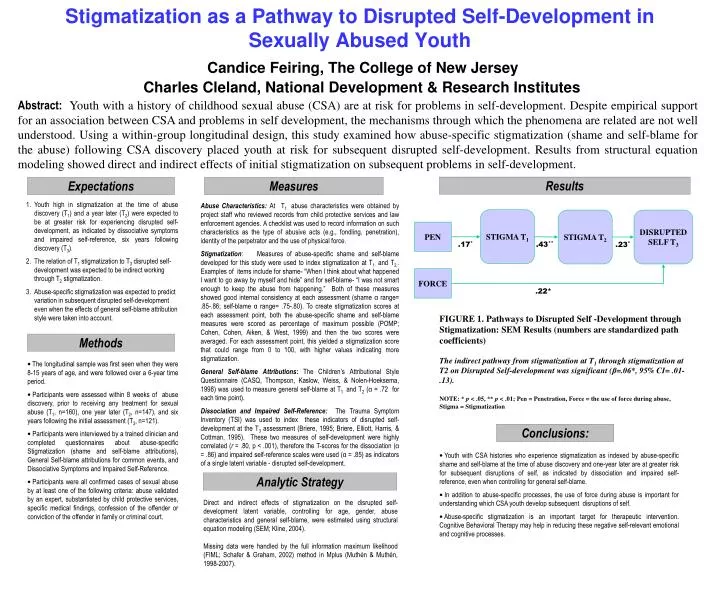
Stigmatization as a Pathway to Disrupted Self-Development inSexually Abused YouthCandice Feiring, The College of New Jersey Charles Cleland, National Development & Research Institutes Abstract:Youth with a history of childhood sexual abuse (CSA) are at risk for problems in self-development. Despite empirical support for an association between CSA and problems in self development, the mechanisms through which the phenomena are related are not well understood. Using a within-group longitudinal design, this study examined how abuse-specific stigmatization (shame and self-blame for the abuse) following CSA discovery placed youth at risk for subsequent disrupted self-development. Results from structural equation modeling showed direct and indirect effects of initial stigmatization on subsequent problems in self-development. Results Expectations Measures • Youth high in stigmatization at the time of abuse discovery (T1) and a year later (T2) were expected to be at greater risk for experiencing disrupted self-development, as indicated by dissociative symptoms and impaired self-reference, six years following discovery (T3). • The relation of T1 stigmatization to T3 disrupted self-development was expected to be indirect working through T2stigmatization. • Abuse-specific stigmatization was expected to predict variation in subsequent disrupted self-development even when the effects of general self-blame attribution style were taken into account. Abuse Characteristics: At T1 abuse characteristics were obtained by project staff who reviewed records from child protective services and law enforcement agencies. A checklist was used to record information on such characteristics as the type of abusive acts (e.g., fondling, penetration), identity of the perpetrator and the use of physical force. Stigmatization: Measures of abuse-specific shame and self-blame developed for this study were used to index stigmatization at T1 and T2.. Examples of items include for shame- “When I think about what happened I want to go away by myself and hide” and for self-blame- “I was not smart enough to keep the abuse from happening.” Both of these measures showed good internal consistency at each assessment (shame α range= .85-.86; self-blame α range= .75-.80). To create stigmatization scores at each assessment point, both the abuse-specific shame and self-blame measures were scored as percentage of maximum possible (POMP; Cohen, Cohen, Aiken, & West, 1999) and then the two scores were averaged. For each assessment point, this yielded a stigmatization score that could range from 0 to 100, with higher values indicating more stigmatization. General Self-blame Attributions: The Children’s Attributional Style Questionnaire (CASQ, Thompson, Kaslow, Weiss, & Nolen-Hoeksema, 1998) was used to measure general self-blame at T1 and T2 (α = .72 for each time point). Dissociation and Impaired Self-Reference: The Trauma Symptom Inventory (TSI) was used to index these indicators of disrupted self-development at the T3 assessment (Briere, 1995; Briere, Elliott, Harris, & Cottman, 1995). These two measures of self-development were highly correlated (r = .80, p < .001), therefore the T-scores for the dissociation (α = .86) and impaired self-reference scales were used (α = .85) as indicators of a single latent variable - disrupted self-development. STIGMA T1 STIGMA T2 DISRUPTED SELF T3 PEN .17* .43** .23* FORCE .22* FIGURE 1. Pathways to Disrupted Self -Development through Stigmatization: SEM Results (numbers are standardized path coefficients) The indirect pathway from stigmatization at T1 through stigmatization at T2 on Disrupted Self-development was significant (β=.06*, 95% CI= .01-.13). NOTE: * p < .05, ** p < .01; Pen = Penetration, Force = the use of force during abuse, Stigma = Stigmatization Methods • The longitudinal sample was first seen when they were 8-15 years of age, and were followed over a 6-year time period. • Participants were assessed within 8 weeks of abuse discovery, prior to receiving any treatment for sexual abuse (T1, n=160), one year later (T2, n=147), and six years following the initial assessment (T3, n=121). • Participants were interviewed by a trained clinician and completed questionnaires about abuse-specific Stigmatization (shame and self-blame attributions), General Self-blame attributions for common events, and Dissociative Symptoms and Impaired Self-Reference. • Participants were all confirmed cases of sexual abuse by at least one of the following criteria: abuse validated by an expert, substantiated by child protective services, specific medical findings, confession of the offender or conviction of the offender in family or criminal court. Conclusions: • Youth with CSA histories who experience stigmatization as indexed by abuse-specific shame and self-blame at the time of abuse discovery and one-year later are at greater risk for subsequent disruptions of self, as indicated by dissociation and impaired self-reference, even when controlling for general self-blame. • In addition to abuse-specific processes, the use of force during abuse is important for understanding which CSA youth develop subsequent disruptions of self. • Abuse-specific stigmatization is an important target for therapeutic intervention. Cognitive Behavioral Therapy may help in reducing these negative self-relevant emotional and cognitive processes. Analytic Strategy Direct and indirect effects of stigmatization on the disrupted self-development latent variable, controlling for age, gender, abuse characteristics and general self-blame, were estimated using structural equation modeling (SEM; Kline, 2004). Missing data were handled by the full information maximum likelihood (FIML; Schafer & Graham, 2002) method in Mplus (Muthén & Muthén, 1998-2007).