Download
1 / 43
430 likes | 614 Views
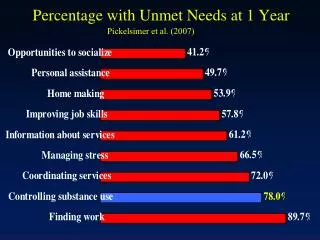
Pickelsimer et al. (2007). Percentage with Unmet Needs at 1 Year. 4 Quadrant Model: Types of Services. High Severity. Quadrant III Substance Abuse System Screening, Accommodation & Linkage. Quadrant IV Specialized TBI & Substance Abuse Services Integrated Programming. Quadrant I

E N D
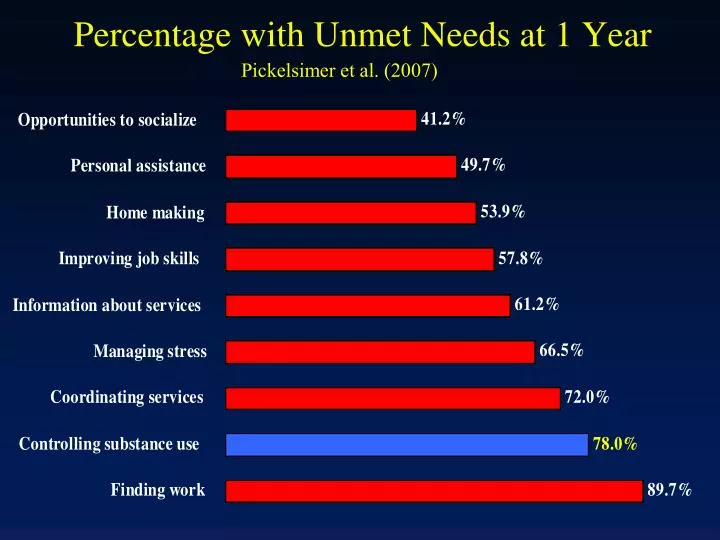
Pickelsimer et al. (2007) Percentage with Unmet Needs at 1 Year
4 Quadrant Model: Types of Services High Severity Quadrant III Substance Abuse System Screening, Accommodation & Linkage Quadrant IV Specialized TBI & Substance Abuse Services Integrated Programming Quadrant I Acute Medical Settings and Primary Care Screening & Brief Interventions Quadrant II Rehabilitation Programs & Services Education, Screening, Brief Interventions & Linkage Substance Use Disorder Low Severity High Severity Traumatic Brain Injury
4 Quadrant Model of Services High Severity Quadrant III Substance Abuse System Screening, Accommodation & Linkage Quadrant IV Specialized TBI & Substance Abuse Services Integrated Programming Quadrant I Acute Medical Settings and Primary Care Screening & Brief Interventions Quadrant II Rehabilitation Programs & Services Education, Screening, Brief Interventions & Linkage Substance Use Disorder Low Severity High Severity Traumatic Brain Injury
Brief Interventions • Brief, opportunistic, counseling and referral conducted in a medical context (e.g., physician’s office, ER, Trauma Program) • For mild to moderate alcohol problems, clinical trials support both efficacy and cost-effectiveness • Most widely published is “FRAMES” developed by Gentilello and colleagues
4 Quadrant Model of Services High Severity Quadrant III Substance Abuse System Screening, Accommodation & Linkage Quadrant IV Specialized TBI & Substance Abuse Services Integrated Programming Quadrant I Acute Medical Settings and Primary Care Screening & Brief Interventions Quadrant II Rehabilitation Programs & Services Education, Screening Brief Interventions & Linkage Substance Use Disorder Low Severity High Severity Traumatic Brain Injury
4 Quadrant Model of Services Quadrant III Substance Abuse System Screening, Accommodation & Linkage High Severity Quadrant IV Specialized TBI & Substance Abuse Services Integrated Programming Quadrant I Acute Medical Settings and Primary Care Screening & Brief Interventions Quadrant II Rehabilitation Programs & Services Education, Screening, Brief Interventions & Linkage Substance Use Disorder Low Severity High Severity Traumatic Brain Injury
% Clients in Substance Abuse Treatment with Histories of TBI
Substance Abuse Treatment Clients Who Have Had a TBI with Loss of Consciousness
TBI among Adolescents in Residential Treatment for Substance Use Disorders • 189 residents of adolescent treatment programs screened at admission • All residents screened during a 5-month period • 3 facilities in Ohio: A=45%; B=23%; C=32% • 70% male, 30% female • 64% white; 30% black; 3% Hispanic; 1% Native American; 2% unknown • Average age= 15.9 years; range=13-18 yrs old; 84% 15-17 yrs old
TBI among participants in IDDT(Corrigan & Deutschle, 2007) • SAMHSA funded Targeted Capacity Expansion grant • Collaborative program in 2 rural counties • 51 program participants (50 included in analyses) • in active treatment in one of the collaborating agencies • previous diagnoses of both a psychiatric and substance use disorder
Persons with TBI face additional challenges seeking substance abuse treatment • It is easy to see behavior as intentionally disruptive, particularly when there are no visible signs of disability: • Frontal lobe damage affects regulation of thoughts, feelings and behavior--promoting disinhibition. • Social “rules” may not be observed and interpersonal cues may not be perceived, creating consternation for fellow clients and staff.
Persons with TBI’s face additional challenges…(cont’d) • Cognitive impairments may affect a person’s communication or learning style, making participation in didactic training and group interventions more difficult. • Misinterpretation of cognitive problems as resistance to treatment undermines treatment relationships.
Two consistent clinical observations: • Substance abuse treatment clients with TBI are more likely to prematurely discontinue treatment, often after being characterized as non-compliant. • There is a greater disconnect between their intention to not use and actual behavior.
4 Quadrant Model: Types of Services High Severity Quadrant IV Specialized TBI & Substance Abuse Services Integrated Programming Quadrant III Substance Abuse System Screening, Accommodation & Linkage Quadrant I Acute Medical Settings and Primary Care Screening & Brief Interventions Quadrant II Rehabilitation Programs & Services Education, Screening, Brief Interventions & Linkage Substance Use Disorder Low Severity High Severity Traumatic Brain Injury
7 Principles of Integrated Treatment for TBI and Substance Abuse • Substance abuse treatment and brain injury rehabilitation are interwoven–not sequential and not just parallel. • Is holistic–addressing all aspects of lifestyle, not just TBI and substance use. • Key staff are skilled in working with both TBI and substance use disorders. • Consumers collaborate with clinicians to develop an individualized treatment plan.
7 Principles of Integrated Treatment for TBI and Substance Abuse (cont’d) 5. Clients go through a process over time in which different services are helpful at different stages of recovery. 6. Clinicians use specific listening and counseling skills to help consumers develop awareness, hopefulness, and motivation for recovery. 7. Smaller staff caseloads, more experienced staff, and long-term treatment usually required.
The OSU TBI Network • Serves persons with cognitive disability due to acquired brain injury who have a substance use disorder. • In existence since 1991, Certified AoD agency in Ohio and CARF accredited as behavioral health program. • Case management model with case finding, education, counseling, resource and service coordination, and consultation with community-based providers. • Resembles Dartmouth model for integrated treatment of co-occurring disorders, except teams are “ad hoc.” • Has been replicated as a free-standing program and as a treatment approach within case management services.
Engagement and retention in treatment is asignificant problem • Successful discharge is intended to include, at least, abstinence, productivity, and improved subjective well-being. • The median length of stay for those discharged with goals met is almost 2 years. • Approximately 1 in 3 clients engaged in treatment are discharged goals met. Effectiveness would be improved by better methods to engage and retain clients in treatment.
Engagement in Treatment(Corrigan, Bogner, Heinemann & Moore, 2005) • 195 subjects; 124 from the TBI Network, 71 from the CAM Program operated by the RRTC on Drugs and Disability at Wright State University. • Conducted during the period from intake to signing an Individualized Service Plan (ISP). • Telephone interviews by staff (other than counselor) immediately following intake. • Primary dependent variable was whether ISP is signed within 30 days (base rate was 45%).
Treatment Conditions • Reduction of barriers to attending appointments • Brief motivational interview to increase motivation for treatment • Financial incentives to participate in treatment • Attention control
Treatment Group Differences in ISP Completion within 30 days
Treatment Group Differences in Number of Missed Appointments
Treatment Group Differences in Premature Termination at 6 months
Retention in Treatment(Corrigan & Bogner, 2007) • 78 subjects from the TBI Network • Conducted after signing first Individualized Service Plan (generally 30-60 days into treatment). • Telephone interviews by staff (other than counselor) immediately following signing the ISP. • Only included Financial Incentive, Barrier Reduction and Attention Control conditions. • Dependent variables were: • Missed appointments in subsequent 30 days • Counselor and Client perceived Therapeutic Alliance at 90 days (HAq-II) • Treatment status at 6 months post-ISP and study completion.
Intervention • Financial Incentive • Barrier Reduction • Attention Control Financial incentives and barrier reductions improve attendance. • Attendance first • 30 days • # missed appts. • Perfect attendance Improved attendance enhances mutually perceived therapeutic alliance. • Therapeutic • Alliance 90 days • Client Haq-II • Counselor Haq-II Greater therapeutic alliance reduces premature termination and increases successful treatment. • Treatment Status • Goals met • Premature termination • Still in treatment
Intervention • Financial Incentive • Barrier Reduction • Attention Control !! Financial incentives and barrier reductions improve attendance. • Attendance first • 30 days • # missed appts. • Perfect attendance Improved attendance enhances mutually perceived therapeutic alliance. • Therapeutic • Alliance 90 days • Client Haq-II • Counselor Haq-II Greater therapeutic alliance reduces premature termination and increases successful treatment. X X • Treatment Status • Goals met • Premature termination • Still in treatment ?
First 10 months of giving gift certificates for engagement in treatment
Employment as a Component of Substance Abuse Treatment • Working is a concrete sign of putting one’s life back together • Need money for self or family • Need to work as a requirement for gaining housing • Need to work as a requirement of probation
The Individualized Placement and Support (IPS) Model IPS is an “aggressive” version of supported employment developed for persons with substance use disorders and severe mental illness
Evidence-Based Principles of IPS • Eligibility is based on consumer choice • Supported employment is integrated with all other aspects of treatment • Competitive employment is the goal • Job search starts soon after a consumer expresses interest in working • Consumer preferences are important in placement • Follow-along supports are continuous IPS for SMI & SUD Clients
Competitive Employment Rates in 12 RCTs of Supported Employment
IPS Study at the TBI Network • 1 of 2 sites conducting study (the other is not exclusively TBI) • Will recruit 96 participants who will be randomly assigned to IPS or standard of care • Outcomes evaluated 3, 6 and 12 months following assignment
Employment Services at the TBI Network Uses IPS model of supported employment Case Manager involves Employment Specialist when client expresses interest in employment Case Manager and Employment Specialist collaborate with client (“Why can’t we go on as three?”) Employment Specialist provides vocational counseling, job development, job placement and employer outreach and education
Ohio Valley Center for Brain Injury Prevention and Rehabilitation www.OhioValley.org www.SynapShots.org