Download
1 / 28
290 likes | 667 Views
Cholera. Rose Lee and Ricardo L é January 14, 2008. Cholera: The Illness. Clinical Features Acute diarrhoeal infection Diarrhoea leads to death by dehydration and kidney failure (stool output can reach 0.5-1L/hour) - hypotension, tachycardia, and vascular collapse.

E N D
Cholera Rose Lee and Ricardo Lé January 14, 2008
Cholera: The Illness Clinical Features • Acute diarrhoeal infection • Diarrhoea leads to death by dehydration and kidney failure (stool output can reach 0.5-1L/hour) - hypotension, tachycardia, and vascular collapse
Short incubation period (2 hours to 5 days) • 75% of those infected do not develop symptoms • 100-1000 organisms may cause disease, although a million are needed to consistently infect
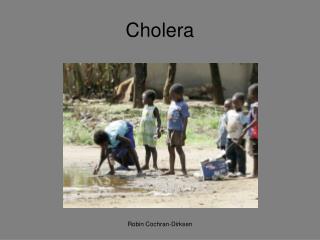
Transmission • Direct fecal-oral contamination or ingestion of contaminated water and food • Linked to inadequate environmental management (lack of safe water and sufficient sanitation) • Human-Human contact does not spread the bacterium
Treatment • Up to 80% of cases can be treated through oral rehydration salts • Severe cases require intravenous fluids (Ringer lactate) • Antibiotics can diminish duration of diarrhoea, reduce volume of rehydation fluids needed, and shorten duration of V.cholerae excretion
Parenteral Vaccine • 2 doses administered 2 weeks apart • Efficacy of approximately 50% • Protection hardly exceeds 6 months • Does not prevent transmission of infectious agent • Not recommended for general public health use
Killed WC/rBS Vaccine • Killed whole-cell V.cholerae in combination with a recombinant B-subunit of cholera toxin • Safe in pregnancy and breastfeeding • Efficacy of approximately 50% after 3 years • Only significant side-effects are mild gastrointestinal disturbances, and toleration is great for HIV-positive subjects
Live, attenuated CVD 103-HgR Vaccine • Protection as early as 1 week after vaccination, with >90% protection against moderate or severe cases • Protection lasts at least 6 months, further data is unknown • Unknown efficacy for children under 2 • No adverse side-effects
Major Issues in Vaccines • Preventative (other measures) • Parenteral: low efficacy, short duration • WC/rBS: 2 doses (logistics) • CVD 103-HgR: Long term results? • Inefficient for O139 or children <2 • Need more tests and trials.
Prevention • Basic health education and hygiene • Mass chemoprophylaxis • Provision of safe water and sanitation • Comprehensive Multidisciplinary Approach: water, sanitation, education, and communication
Control of Spread • Set up treatment centres for prompt treatment. • Sanitary measures. • Comprehensive surveillance data (adapt to each situation) for a comprehensive multidisciplinary approach.
Vibrio Cholerae The Organism
Type of Bacterium • Gram negative (LPS cell wall) • Type of Gammaproteobacteria • Distinguishing factors: Oxidase-positive, motile via polar flagellum, and both respiratory and fermentative metabolism. • Simple growth requirements
History of Cholera • First observed in India then S. Asia • Discovered conclusively in 1883 by Koch • Spread to Europe and Americas from 1817. 6 epidemics by 1990s. • 7th epidemic in 1961 of El Tor biotype • Spread across Asia, Middle East, Africa, and parts of Europe
Some Definitions: • Strain: Subset of a bacteria differing from same species. • Biotype:Same genotype, but different phenotype. • Serotype: Closely related microorganisms distinguished by a characteristic set of antigens.
Many strains of Vibio cholerae. • O antigens distinguish 139 serotypes: O1 (3 biotypes—each has “classical” or El Tor phenotype), O139 Bengal. • O139 is a new serological strain with unique O-antigen (no residual immunity from O1)
Differences • El Tor strain is more virulent (replacing classical): • Lower ratio of cases to carriers • Longer duration of carriage after • Survives longer in extraintestinal env • O139 Bengal (derived from El Tor) • Different antigenic structure on LPS • Distinct polysaccharide capsule • Possess all El Tor virulence
Virulence Factors • Cholera toxin • Tcp pili • Aggregation, adhesion • Flagellum • withstand propulsive gut • Resistant to bile salts in intestines • If escapes low pH of stomach, easy to survive in intestines
Cholera toxin • Potent exotoxin • multimeric protein complex of five binding subunits (B) and one enzymatic (A) subunit. • B subunits bind to intestinal epithelia cell and A1 subunit enter cell and activates adenylate cyclase enzyme.
A1 catalyzes ADP-Ribose attachment to Gs Gi cannot hydrolyze GTP to inactivate adenylate cyclase. • cAMP produced at high rate. Triggers Cl- into intestines. • H2O, Na+, bicarbonate, and other electrolytes follow
Colonization • Adhesins • Tcp pili, hemagglutinin, acf gene products • Neuraminidase • Motility • Chemotaxis • Toxin production
Regulation • Enterotoxin is a product of ctx genes regulated by transcription • Environmental signals -Temperature, pH, osmolarity, amino acids • ToxR regulatory protein activated -Induces positive control, binds to DNA • Genes for attachment and toxin production transcribed
Ecology • Can exist in dormant state • Conversion to infectious state: -increase Temp, pH, nutrients. -decrease salinity • Can shift to “rugose form”: exopolysaccharide production for cell aggregation, resists chlorine
On our mission we came across a village in rural Bangladesh. It is very small but very crowded with poor water sanitation and irrigation systems. Its position is dangerously close to the urban slums that have had cholera outbreaks within the past few months. Luckily, there has been no reported cases of cholera so far within the last 6 months… but now we have some decisions to make.
Discussion Question 1 • What is our plan of action in regards to this village? • Where should the emphasis be placed on protecting a population before an outbreak occurs? Vaccination or sanitation? • What are the pros and cons of each?
Discussion Question 2 • Unfortunately, while the members were debating, an outbreak occurred in this village. What is the plan now? -What is the best hybrid solution for controlling a cholera outbreak? You have short time and limited resources.
Discussion Question 3 • The outbreak has been controlled for the moment. What should be the long-term plan for this population?
Discussion Question 4 • What are your sentiments and policies regarding cholera around the world? How do you feel about the importance each of these as aspects? • Scientific Lab Research • Field Work • Infrastructure of Sanitation • Education