Download
1 / 56
1.07k likes | 2.74k Views
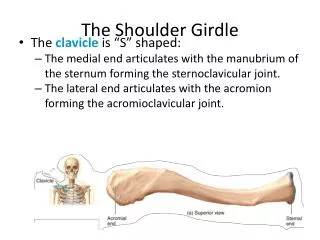
Shoulder Girdle Joint Injection Workshop. Virginia Osteopathic Medical Association 2011 Fall CME Conference Hotel Roanoke & Conference Center Roanoke, Virginia September 23, 2011 Bradley M. McCrady, DO Fellow, Primary Care Sports Medicine

E N D
Shoulder Girdle Joint InjectionWorkshop Virginia Osteopathic Medical Association 2011 Fall CME Conference Hotel Roanoke & Conference Center Roanoke, Virginia September 23, 2011 Bradley M. McCrady, DO Fellow, Primary Care Sports Medicine Edward Via College of Osteopathic Medicine- Virginia Campus Virginia Polytechnic Institute and State University
Objectives • Identify indications and contraindications for joint injections of the shoulder girdle. • Review necessary equipment of shoulder injections. • Discuss techniques to perform various shoulder girdle injections. • Illustrate techniques of ultrasound-guided injections of the shoulder girdle. • Demonstrate skills to perform various common shoulder girdle injections.
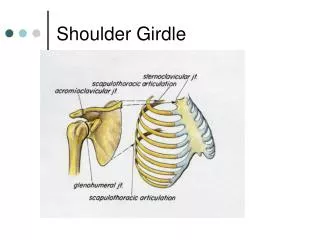
Shoulder Complex • Shoulder is a complicated anatomical and biomechanical joint • “Fragile Equilibrium” • Multiple joints • Static and dynamic stabilizers Hoppenfeld, S. Physical Examination of the Spine and Extremities. Prentice Hall; 1976 http://www.sportfit.com/tips/rotatorcuff/images/Z4rtrs.gif
What Providers Need to Know About Joint Injection and Aspiration • Relatively simple procedure • Complications are uncommon • Injection/arthrocentesiscan provide diagnosis, relieve pain, decrease joint damage • “Liquid biopsy of joint” • Useful information can be provided by relatively inexpensive tests • Can help differentiate inflammatory from non-inflammatory arthritis • Judicious use of anesthetics and steroids may be safer than systemic medications • Summary There are often more reasons for doing than not in the right clinical scenario
Indications for Joint Injection/Aspiration • Diagnostic • Acute inflammatory arthritis (24-48 hours) in a patient who has never had these symptoms before • Acute effusion in the setting of fever, chills, or presence of infection at another site • Acute effusion in the setting of trauma • Prior to committing patients to long-term, expensive or toxic therapy • Therapeutic • Provide for a better musculoskeletal exam (i.e. pain control) • To suppress inflammation in one or two isolated joints • Adjuvant therapy to a few joints resistant to systemic therapy • To facilitate a rehabilitative therapy program • To support a patient with active joint inflammation pending the effects of systemic therapy • To remove exudative fluid from a septic joint • To relieve pain in a swollen joint
Conditions Likely to be Improved by Joint or Periarticular Injections • Rheumatoid arthritis • Seronegativespondyloarthropathies • Crystal induced arthritis • Carpal tunnel • Bursitis • Tenosynovitis/tendinitis • Adhesive capsulitis • Osteoarthritis
Contraindication to Joint Injection/Aspiration • Absolute • Uncooperative patient • Allergy to anesthesia or steroid (very rare) • Lack of informed consent • Injection through infected tissues • Previous severe steroid flare • Injection of steroid into critical weight-bearing tendons • Relative • Injection near critical structures • Coagulation disorders • Uncontrolled diabetes • h/o AVN • Previous joint replacement at injection site • More than 3 previous steroid injections in a major weight bearing joint in the preceding year • Concern to activate any latent disease • Excessive anxiety
Equipment • Informed consent • Non-sterile exam gloves • Marking pen • Alcohol pads +/- povidine-iodine • Gauze pads • Syringe(s) • Needle • Anesthetic • Steroid • Adhesive bandages McNabb, James. A Practical Guide to Joint & Soft Tissue Injection & Aspiration. 2nd Ed.LWW; 2010.
Safety First • Position for comfort! • Define anatomy • Universal precautions • Vaccines • Gown and mask not necessary • Clean vs sterile technique • Aspirate prior to injections • Do not recap needles • Proper disposal of equipment • Observe patient in office following injection for 15-30 min Baima, J.Curr Rev Musculoskelet Med (2008) 1:88–91 Hemani, M. Rev Urol. 2009;11(4):190-195 Darouiche, RO. N Engl J Med 2010;362:18-26
Topical Preparation • Infection is not common • Actual reported incidence is unknown, but is thought to vary from 1: 3,000 to 1:50,000 • 70% isopropyl alcohol vs 10% povidone-iodine • Ethyl chloride fine spray may have antimicrobial activity http://www.shopmedrx.com/qt_images/TRI_103201.jpg http://sani-system.com/images/products/b15901.jpg http://www.gebauerco.com/Images/picEthylChlorideLeft.gif Baima, J.Curr Rev Musculoskelet Med (2008) 1:88–91 Hemani, M. Rev Urol. 2009;11(4):190-195 Darouiche, RO. N Engl J Med 2010;362:18-26 Clinical Radiology, Volume 61, Issue 12, Pages 1055-1057
Steroids-History • Hydrocortisone acetate was first introduced in the 1949 for Rheumatoid arthritis by Hollander • “No other form of treatment has given such consistent local symptomatic relief in so many for so long with so few harmful effects.” • Oriole baseball pitcher Jim Palmer • “…cortisone is a miracle drug ... for a week!" • Long history of use in athletics • Treat the secondary inflammation • Need to find the cause Nepple, J. Sports Health: A Multidisciplinary Approach 2009 1: 396-404 Leadbetter WB. Clin Sports Med.1995;14(2):353-410.
Steroids-Physiology • Stabilizing lysosomal membranes of inflammatory cells • Decreasing local vascular permeability • Altering neutrophilchemotaxis and function • Able to pass through cell membranes and bind to nuclear steroid receptors • Where they influence RNA transcription Nepple, J. Sports Health: A Multidisciplinary Approach 2009 1: 396-404
Steroids-Use • Hill et al surveyed members of the American Academy of Orthopaedic Surgeons on use of corticosteroids • 90% of used corticosteroid injections • Performed an average of 150 intra-articular and 193 extra-articular injections per year • Conditions warranting injection • Epicondylitis (93%) • Shoulder bursitis (91%) • Greater trochanteric bursitis (91%) • DeQuervain’s tenosynovitis (87%) • Bicipital tendonitis (81%) Hill JJ Jr,. ContempOrthop. 1989;18:39-45. McNabb, James. A Practical Guide to Joint & Soft Tissue Injection & Aspiration. 2nd Ed.LWW; 2010.
Anesthetics • Decrease nerve conduction through the blockade of Na channels, which disrupts axonal nerve conduction • Typically steroid agent is combined with a local anesthetic agent • Decrease the pain • Dilute the steroid • Increase the distribution of the agent to the treated area • Lidocaine • Rapid onset (minutes) • Short duration (60-90 minutes) • Bupivicaine • Slower onset (30 minutes) • Longer duration (6-8 hours) • Buffering • Sodium bicarbonate Nepple, J. Sports Health: A Multidisciplinary Approach 2009 1: 396-404
What Patients (and Providers) Need to Know about Joint Injection • Relief will typically last weeks or longer • Avoid injecting ligamentous or tendon structure directly • Activity modification following injections of steroids is uncertain • Maximal number of injections and the required period between injections have not been determined Nichols, A Clin J Sport Med 2005;15(5) : E370 Pfenninger JL. Procedures for primary care physicians. St. Louis: Mosby, 1994.
What Patients (and Providers) Need to Know about Joint Injection • In a meta-analysis summarizing 25+ studies, they noted a 5.5% complication rate • The most common side effects included skin atrophy (2.4%), skin depigmentation (0.8%), localized erythema and warmth (0.7%), and facial flushing (0.6%) • Post-injection pain was noted in up to 9% of patients • Post injection flare (2-5%) • Prolonged and repeated usage may increase the risk of complications and systemic side effects • In diabetic patients, hyperglycemia has been shown to persist up to 5 days after a single soft tissue injection (very low risk) Dietzel, D Current Sports Medicine Reports 2004, 3:310–315 Nepple, J. Sports Health: A Multidisciplinary Approach 2009 1: 396-404 Wang AA. J Hand Surg [Am]. 2006;31(6):979-981. Pfenninger, JL Procedures in Primary Care 2nd Ed. 2003: 1479-1499
Typical Injection/Aspiration Procedure • Determine the medical diagnosis and consider relevant differential diagnoses • Discuss the proposed procedure and alternatives with the patient • Obtain written informed consent from the patient • Collect and prepare the required materials • Correctly position the patient for the procedure • Identify and mark the anatomic landmarks and injection site with ink • Do not allow the patient to move the affected area from the time that the marks are placed until after the procedure is completed • Press firmly on the skin with the retracted tip of a ballpoint pen to further identify the injection site • Prepare the site for injection by cleansing with a topical antimicrobial agent (povidine-iodine and/or alcohol swab) • If using the povidone, allow to dry for full antibacterial effect • Provide local anesthesia as indicated through use of tactile distraction, vapocoolant spray (ethyl chloride or PainEase), and/or injected local anesthesia McNabb, James. A Practical Guide to Joint & Soft Tissue Injection & Aspiration. 2nd Ed.LWW; 2010. Pfenninger, JL Procedures in Primary Care 2nd Ed. 2003: 1479-1499
Typical Injection/Aspiration Procedure • Using the no-touch technique, introduce the needle at the injection site and advance into the treatment area • Aspirate fluid (optional) using a 18 or 20-g needle and send it for laboratory examination if indicated • If injecting corticosteroid immediately following aspiration, do not remove the needle from the joint or bursa; In this case, grasp the needle hub firmly (with a hemostat clamp if necessary), twist off the original syringe, and then immediately attach the second syringe that contains the corticosteroid • Always aspirate before injection to avoid intravascular administration • Inject corticosteroid solution into the treatment area • If not aspirating then use 25-g needle • Do not inject the medication against resistance • Withdraw the needle • Apply direct pressure over the injection site with a gauze pad • Apply an adhesive dressing • Provide the patient with specific post-injection instructions McNabb, James. A Practical Guide to Joint & Soft Tissue Injection & Aspiration. 2nd Ed.LWW; 2010. Pfenninger, JL Procedures in Primary Care 2nd Ed. 2003: 1479-1499
Informed Consent • Patient’s consent to allow provider (and his/her pupils) to perform the procedure. • All alternative treatments discussed with the patient in lieu of procedure. • Benefits and risks to the procedure. • Explanation of the procedure in lay language to the patient. • Signature of the patient or authorized representative, witness, and provider.
Shoulder Girdle Injections • Subacromial • Posterior • Lateral • Glenohumeral • Posterior • Anterior • Acromioclavicular • Sternoclavicular • Biceps brachii long head
Subacromial Injection Lateral Approach • Find lateral edge of acromion and mark • Palpate soft spot below the acromion and above the humeral head • Insert needle perpendicular through the deltoid towards the bursa
Subacromial Injection Posterior Approach • Find lateral edge of the acromion and mark • Palpate posterior edge of the acromion and mark • Find posterolateral edge of the acromion and mark a spot 2 cm below the corner McNabb, James. A Practical Guide to Joint & Soft Tissue Injection & Aspiration. 2nd Ed.LWW; 2010. Seroyer, S. Sports Health 2009; 1 (2): 108-120
Subacromial Injection Posterior Approach • Position the needle at a 30 ° angle to the skin with the needle tip directed cephalad toward the acromion • Insert the needle getting underneath the acromion and advance until the needle tip touches the undersurface of the acromion • Once at the acromion, back off 1-2mm
Glenohumeral Injection Posterior Approach • Find lateral edge of acromion • Palpate the posterior edge of the acromion • Mark spot 2 cm below posterior lateral corner • Target is coracoid process
Glenohumeral Injection Posterior Approach • Advance needle towards coracoid process until tip touches humeral head and retract needle 1-2mm
Glenohumeral Injection Anterior Approach • Identify coracoid process • Injection point is 1 cm lateral to the coracoid
Glenohumeral Injection Anterior Approach • Insert needle perpendicular to the skin toward the target 2 cm caudad to the posterior lateral corner of the acromion • Advance needle until it reaches the humeral head and retract 1-2mm
Long Head Biceps Injection • Palpate course of biceps long head tendon with the patient flexing the elbow • Palpate location of maximal tenderness which is usually under the edge of the pectoralis major http://www.aafp.org/afp/2009/0901/afp20090901p470-f1.jpg
Long Head Biceps Injection • Position needle at a 45° angle to the skin with needle directed proximally • Advance needle until needle tip touches tendon, back needle off 1-2mm • Medication should flow smoothly
Acromioclavicular Injection • Identify AC joint by palpating the clavicle in a medial to lateral direction until reaching a small depression that may be tender http://upload.wikimedia.org/wikipedia/commons/thumb/3/3b/Gray326.png/250px-Gray326.png
Acromioclavicular Injection • Insert needle perpendicular to the skin with the needle tip directed caudad
Sternoclavicular Injection • Identify SC joint by palpating the clavicle in a lateral to medial direction until reaching a small depression that will likely be tender
Sternoclavicular Injection • Insert needle perpendicular to the skin and advance into SC space
Musculoskeletal Ultrasound • The use of high-frequency sound waves (3-17MHz) to image soft tissues and bony structures in the body for the purpose of diagnosing pathology or guiding real-time interventional procedures http://cdn.bleacherreport.com/images_root/image_pictures/0236/5499/39664_crop_340x234.jpg Pinzon, EG and Moore, RE. Musculoskeletal Ultrasound: a brief overview of diagnostic and therapeutic application in musculoskeletal medicine. Practical Pain Management. June 2009.
Ultrasound Terminology • Echogenecity- the ability of tissue to reflect ultrasound waves back toward the transducer and produce an echo. (The higher the echogenicity of tissues, the brighter they appear on ultrasound imaging) • Hyperechoic- seen as brighter on ultrasound relative to surrounding tissues due to higher reflectivity of the US beam • Isoechoic- structures are seen as bright as surrounding structures on conventional US imaging due to similar reflectivity to the US beam Pinzon, EG and Moore, RE. Musculoskeletal Ultrasound: a brief overview of diagnostic and therapeutic application in musculoskeletal medicine. Practical Pain Management. June 2009.
Ultrasound Terminology • Hypoechoic- structures are seen as darker relative to the surrounding structures on US imaging due to the US beam being reflected to a lesser extent • Anechoic- structures that lack internal reflectors fail to reflect the US beam to the transducer and are seen as homogenously black on imaging • Anisotrophy- the effect of the beam not being reflected back to the transducer when the probe is not perpendicular to the structure being evaluated Pinzon, EG and Moore, RE. Musculoskeletal Ultrasound: a brief overview of diagnostic and therapeutic application in musculoskeletal medicine. Practical Pain Management. June 2009.
Ultrasound Terminology • Transverse- cross sectional view • Sagittal (Longitudinal)- long axis plane view • Coronal- long axis plane view dividing anterior and posterior http://www2.healthsci.tufts.edu/saif/Vevo2100/Ultrasound-Terminology.pdf
Ultrasound Equipment • High Resolution Machine • Transducers • Linear 8-14 MHz • Curvilinear 2-5 MHz • “Hockey Stick” • Printer • CD/DVD/USB unit Schaefer, MP. Ultrasound Guided Interventions in PM&R. MRIO PM&R Grand Rounds. 9 November 2009. http://www.ucsdultrasound.com/yahoo_site_admin/assets/images/ultrasound_transducers.24673744_large.jpg
Ultrasound Guidance Advantages • Real-time guidance • Assess anatomy • Soft tissue visualization • Visualize neurovascular structures • No radiation Schaefer, MP. Ultrasound Guided Interventions in PM&R. MRIO PM&R Grand Rounds. 9 November 2009.
Ultrasound Guidance Limitations • Obesity (depth ~6cm) • No contrast confirmation • No visualization deep to bony structures (very limited use in spine injections) • Operator dependency • Superficial tenderness Schaefer, MP. Ultrasound Guided Interventions in PM&R. MRIO PM&R Grand Rounds. 9 November 2009.
Equipment for U/S Guided Injections • Informed consent • Sterile vs non-sterile gloves? • Marking pen • Alcohol pads • Povidine-iodine • Gauze pads • Syringes • Needles (typically longer than non-guided injections) • Echoblock needle? • Sterile transducer cover? • Sterile gel • Anesthetic • Steroid • Adhesive bandages Schaefer, MP. Ultrasound Guided Interventions in PM&R. MRIO PM&R Grand Rounds. 9 November 2009.
Subacromial Injection http://www.essr.org/html/img/pool/shoulder.pdf Schaefer, MP. Ultrasound Guided Interventions in PM&R. MRIO PM&R Grand Rounds. 9 November 2009.
Subacromial Injection Schaefer, MP. Ultrasound Guided Interventions in PM&R. MRIO PM&R Grand Rounds. 9 November 2009.
Acromioclavicular Injection http://www.essr.org/html/img/pool/shoulder.pdf
Acromioclavicular Injection Schaefer, MP. Ultrasound Guided Interventions in PM&R. MRIO PM&R Grand Rounds. 9 November 2009.
Glenohumeral Injection http://www.essr.org/html/img/pool/shoulder.pdf
Glenohumeral Injection Schaefer, MP. Ultrasound Guided Interventions in PM&R. MRIO PM&R Grand Rounds. 9 November 2009.
Long Head Biceps Brachii Injection http://www.essr.org/html/img/pool/shoulder.pdf