Download
1 / 55
570 likes | 807 Views
Clostridium difficile: 2012 Update. Julia B. Garcia-Diaz, MD, MSc Ochsner Clinic Foundation October 20 th , 2012. Case Presentation . 61 yo male was admitted to the hospital with the complain of bloody diarrhea

E N D
Clostridium difficile: 2012 Update Julia B. Garcia-Diaz, MD, MSc Ochsner Clinic Foundation October 20th, 2012
Case Presentation • 61 yo male was admitted to the hospital with the complain of bloody diarrhea • 4 days before admission, he was diagnosed with gastroenteritis (fever 39.5, diarrhea) and was given ciprofloxacin. In spite of taking the antibiotics, he continued to pass watery stool mixed with blood • Past history: liver disease with esophagealvarices for which band ligation was done twice & also pancytopenia due to hypersplenism
Laboratory • Stool: WBC 5-10/HPF, RBC 10-20/HPF. • Positive stool occult blood • Stool Clostridium difficile: positive • CBC • WBCs 2.1 x 103 /cm • Hemoglobin 10.8 gm/dl • Hematocrit 31.2 • Platelet count 36,000
Phosphorus 2.9 mg/dl Calcium of 8.2 mg/dl Albumin 2.3 gm/dl Alkaline phosphatase83 U/L AST 21 U/L ALT 18 U/L GGT 18 U/L Total Bilirubin 2.9 mg/dl Laboratory • Direct1.8 mg/dl • BUN 27 mg/dl • Creatinine 0.7 mg/dl • Sodium 133 mEq/L • Potassium 3.3 Meq/L
Abdominal ultrasound showed shrunken cirrhotic liver measuring 12 cm Gallbladder showed small stones. The spleen was hugely enlarged measuring 19.98 x 7.77 cm
Hospital Course • The patient was started on oral vancomycin 250mg q6h and metronidazole treatment 500mg q8h • 4 days later: the patient started complaining of severe abdominal pain and examination showed markedly distended abdomen with evidence of guarding and rigidity • A KUB was done and it showed marked distension of the colon reaching up to 9.5 cm in diameter
Hospital Course • A cecostomy tube was placed in to help in deflation of the colon followed by sigmoidoscopy or total colonoscopy.
Hospital Course • The patient had successful insertion of cecostomy tube and sigmoidoscopy was performed with improvement of the abdominal distension
Hospital Course • Rapid deterioration with hepatic coma and hepatorenal failure occurred. • 4 days later the patient died.
AN EPIDEMIC, TOXIN GENE STRAIN OF CLOSTRIDIUM DIFFICILEMcDonald LC. NEJM 2005;353:1433 • Reported increase 2000-01 – 21% • Pittsburgh – 26 colectomies and 18 deaths
CONCLUSIONS C. difficile appears to be causing more disease and more serious disease. Possible role of strain BI/NAP1 • Toxin A and B – high production
C.L. McDonaldDale Gerding • 23 states and 5 countries • 2004: diagnosis (ICD-9) showed 25% increase over 2003 • Average rate is 5-10/1000 discharges (US hospitals) • Guidelines (SHEA/IDSA): Spring ’07 • Antibiotics: cephalosporinsand FQ • NAP-1 strain: reference lab CDC if epidemic in new area • Strain does not change management
A PREDOMINANTLY CLONAL MULTI-INSTITUTIONAL OUTBREAK OF CLOSTRIDIUM DIFFICILE-ASSOCIATED DIARRHEA WITH HIGH MORBIDITY AND MORTALITYLooV. NEJM 2005;353:2442 METHOD: Prospective study in 12 Quebec hospitals • Risk factors • Clinical features • Strain types: PFGE, binary toxin, tcdC deletion
Main intervention: • Infection control • Single rooms, contact precautions, early detection and Rx, dedicated equipment, soap, household bleach and education • Antibiotic control 5-10% decrease • Toxin assay: cytotoxinat 24 hr • Treatment: metronidazolein ~ 80% • Rates in 12 hospitals consortium and region decrease >50%
Voluntary laboratory reports of C. difficile positive faecal specimens: England, Wales and Northern Ireland* 1990 - 2011
Increase in Clostridium difficile–related Mortality Rates, United States, 1999–2004
The First Case • 22 year old female, patient of Dr. William Osler • “A miserable, emaciated creature in a wretched physical condition.” • Underwent surgical resection of a gastric tumor on August 26, 1892 • Postoperatively developed diarrhea that became progressively more severe • Died on post op day 15 “Diphtheritic membrane”
History Cont’d A fatal case of pseudomembranous colitis in 1948 was linked to streptomycin use, led to reexamination of the 1892 case “Myriads of gram positive cocci” found- Staphylococcus aureus postulated as cause Studies in 1950’s and 60’s document an association but did not prove causation
History • Clostridium difficile was first described in 1935, but its association with disease was not identified until 1978.
Microbiology • An anaerobic, spore forming gram positive rod; first described as a member of the normal flora of healthy infants in 1935 • Due to the difficulty in cultivating the organism, it was originally called Bacillus difficilis • Given its current name 3 years later
Toxin Production • 5-25% of strains do not produce toxins and don’t cause disease • Toxin A • 308 kdenterotoxin and cytotoxin • Chemoattractant for neutrophils • Activator for macrophages and mast cells • Toxin B • 269 kd potent cytotoxin • Disrupts the actin cytoskeleton • Found to be a potent necrotizing enterotoxin • Probably acts synergistically with toxin A
Epidemiology • The most common recognized cause of nosocomial diarrhea • Incidence and severity increasing: • A new strain has been identified that carries and additional toxin (iota toxin) • C. difficile acquiring resistance to more antimicrobials • Frequency varies by institution • Results in 3.6 excess hospital days, cost of $3,700/pt • Readmissions for CDAD cost $128,000 per hospital per year • Conservative estimate of US cost per year $1.1 billion
Acquisition of the Organism • In healthy adults intestinal carriage rates of toxigenicC. difficile are 5% or less • Carriage in healthy adults thought to be transient • High prevalence in newborns- up to 60-70%- all asymptomatic • In hospitalized patients colonization begins upon admission in patients given antimicrobials • 13-20% within the first week • 50% in patients hospitalized for more than 4 weeks • Even relatively minute amounts of antimicrobials can predispose to colonization
Pathogenesis of Infection • Three critical events necessary for CDAD • Disruption of the normal colonic microflora by antimicrobials or other means • Ingestion by the patient of a toxigenic strain of C. difficile and its arrival intact in the lower GI tract • One or more additional requirements for developing invasive disease • Advancing age • Severe underlying disease of any kind • Prolonged hospital stays • Manipulation of the GI tract (NG tubes, enemas, surgery, motility altering drugs) • Acid neutralizing drugs
Medications Associated with C. difficile • Most common antimicrobials • Clindamycin • Ampicillin/amoxicillin • Cephalosporins • Fluoroquinolones • Infrequent- Tetracyclines, macrolides, TMP/SMX • Rare or never- IV aminoglycosides, metronidazole, vancomycin, bacitracin • Chemotherapeutics with antibacterial activities • Ifosfamide, carboplatinetoposide 8% incidence • Others Mtx, 5FU, doxorubicin, cyclophosphamide • Bowel preparation regimens
Clinical Disease Spectrum • Asymptomatic colonization 2-5 or more X more common than clinical illness of any type • Mild diarrhea, minimal discomfort • Typical CDAD: • Crampy abdominal pain • Profuse diarrhea with mucoid, greenish watery stool with a characteristic odor • Low grade fever and leukocytosis • More severe disease with high fever, marked leukocytosis
Disruption of protective colonic flora (AB or AN) Colonization with toxigenic C. difficile by fecal-oral transmission Toxin A and B production A/B: Cytoskeletal damage, loss of tight junctions. A: Mucosal injury, inflammation, fluid secretion. Colitis andDiarrhea
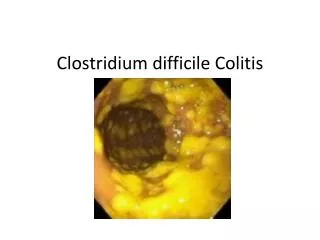
Diagnosis • Endoscopy (pseudomembranous colitis) • Culture • Cell culture cytotoxin test • EIA toxin test • PCR toxin gene detection
Diagnosis • Endoscopy looking for pseudomembranes • Quick, and specific • Pseudomembrane formation usually starts on the right side • Pseudomembrane formation a late manifestation • Culture • Takes several days • Need cytotoxic assay of organism after culture • Immunoassays
EIA toxin tests • Can detect toxin A, toxin B, or both • Rapid, cheap, and specific • Less sensitive than cytotoxin test • Toxin A tests will miss rare C. difficile isolates that produce toxin B only (Toxin A-negative, toxin B-positive outbreak, Winnipeg, 1998)
Treatment • General principles • Whenever possible withdraw the offending antibiotic • Be patient; some improvement seen in first 2 days but mean time until resolution of diarrhea is 2-4 days • Don’t call them nonresponders until 6 days of therapy • Treat for 10 days • Avoid antiperistaltic agents • No role for test of cure assays
Metronidazole • MIC 90of 0.4 ug/ml vs. C. difficile • 98% cure rate documented • Well absorbed in the upper GI tract: in healthy volunteers fecal concentration of drug low to undetectable • Bactericidal fecal concentrations achieved in the stool of patients with CDAD: fecal concentrations decrease as diarrhea improves • Drug secreted directly across inflamed mucosa • Decreased intestinal transit time with diarrhea decreases absorption
Vancomycin MIC 90of 1.6 ug/ml Fecal concentrations of 2,000 to 5,000 ug/ml with po drug Cure rates 98-100% Second line therapy due to concerns of selecting for vancomycin resistant Enterococcus (VRE) No drug in GI tract when given IV Can be given by enema
A Comparison of Vancomycin and Metronidazole for the Treatment of Clostridium difficile–Associated Diarrhea, Stratified by Disease Severity Zar et al. Clinical Infectious Diseases 2007; 45:302–7
Treatment of Multiple Relapses No controlled studies, lots of anecdotes and “personal favorite” regimens Tapering courses of vancomycin or metronidazole Vancomycin plus rifampin Rifaximin chasers Yogurt or other Lactobacillus preparations Saccharomycesboulardii plus antibiotics Intravenous immune globulin Cholestyramine with or without antimicrobials