Download

1 / 44
500 likes | 1.57k Views
Liver dysfunction and Drugs metabolism. Dr V.Sebghatollahi Isfahan university of medical science. Liver Functions:. Metabolism – Carbohydrate, Fat & Protein Secretory – Bile acids, bile salts & pigments Excretory – Bilirubin , drugs, toxins Synthesis – Albumin, coagulation factors

E N D
Liver dysfunctionand Drugs metabolism Dr V.Sebghatollahi Isfahan university of medical science
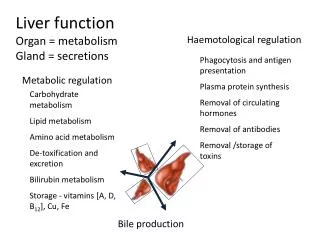
Liver Functions: • Metabolism – Carbohydrate, Fat & Protein • Secretory– Bile acids, bile salts & pigments • Excretory – Bilirubin, drugs, toxins • Synthesis – Albumin, coagulation factors • Storage – Vitamins, carbohydrates etc. • Detoxification – toxins, ammonia, etc.
Introduction • Cirrhosisis common end result of many chronic liver disorders. • Inflammtion – healing with fibrosis - Regeneration of remaining hepatocytes form regenerating nodules. • Loss of normal architecture & function.
INTRODUCTION • It is generally considered to be irreversible in its advanced stages at which point the only option may be liver transplantation. • However, reversal of cirrhosis (in its earlier stages) has been documented in several forms of liver disease following treatment of the underlying cause.
Etiology of Cirrhosis • The most common causes of cirrhosis in the United States are: • hepatitis C • alcoholic liver disease • Nonalcoholic fattyliver disease • which together accounted for approximately 80 percent of patients on the liver transplantation waitlist between 2004 and 2013
Etiology of Cirrhosis • In developed countries, common causes of cirrhosis include : • Chronic viral hepatitis (hepatitis B, C) • Alcoholic liver disease • Hemochromatosis • Nonalcoholic fatty liver disease
Pathogenesis: • Hepatocyte injury leading to necrosis. • Alcohol, virus, drugs, toxins, genetic etc.. • Chronic inflammation - (hepatitis). • Bridging fibrosis. • Regeneration of remaining hepatocytes Proliferate as round nodules. • Loss of vascular arrangement results in regenerating hepatocytes ineffective.
Clinical Features • Hepatocellular failure. • Malnutrition, low albumin & clotting factors, bleeding. • Hepatic encephalopathy. • Portal hypertension. • Ascites, Porta systemic shunts, varices, splenomegaly.
Physical examination • Spider angiomas • Palmarerythema • Nail changes • Muehrcke's nails • Terry’s nails • Gynecomastia • Testicular atrophy
Muehrcke's nails Terry’s nails Clinical Manifestations
Conclusions: • Common end result of diffuse liver damage. (Viral hepatitis, Alcohol, congenital, drugs, toxins & Idiopathic) • Characterised by diffuse loss of architecture. • Fibrous bands & regenerating nodules distort and abstruct blood flow. (inefficient function) • Hepatocellular insufficiency & portal hypertension. • Shrunken, scarred liver, ascitis, spleenomegaly, liver failure, CNS toxicity.
Metabolism • The metabolism of drugs and other xenobiotics into more hydrophilic metabolites is essential for the elimination of these compounds from the body and termination of their biological activity.
Types of Metabolism • Phase 1 Reactions • usually convert the parent drug into a more polar metabolite by introducing or unmasking a functional group (-OH, -NH2, -SH). Metabolite is usually inactive. • Phase 2 Reactions - Conjugation • an endogenous substrate (glucuronic acid, sulfuric acid, acetic acid, or amino acid) is attached to a functional group on the drug or phase I metabolite.
Absorption Elimination Metabolism Lipophilic Hydrophilic Phase I Phase II conjugate Drug Drug metabolite with modified activity conjugate Drug Inactive drug metabolite conjugate Drug
Biotransformation • Generates more polar (water soluble), inactive metabolites • Readily excreted from body • Metabolites may still have potent biological activity (or may have toxic properties) • Generally applicable to metabolism of all xenobiotics as well as endogenous compounds such as steroids, vitamins and fatty acids
First-Pass Metabolism • Following nonparenteral administration of a drug, a significant portion of the dose may be metabolically inactivated in either the intestinal endothelium or the liver before it reaches the systemic circulation • Limits oral availability of highly metabolized drugs
Liver disease may have complex effects on drug clearance, biotransformation, and pharmacokinetics
There is no easily available measure of liver function, with the "liver function tests" such as AST, ALT, GGT & alkaline phosphatase providing an indication of liver cell damage rather than ability of the liver to metabolise drugs. • This contrasts with renal disease, where estimates of renal function based on creatinine clearance correlate with renal drug elimination.
Type of Disease • In liver disease the type of disease does matter: • Hepatitis – not much effect • Biliaryobstruction – not much effect (initially) • Cirrhosis – has major effects on drug handling • Liver Dysfunction can lead to impaired drug metabolism-decreased enzyme activity • First pass metabolism effected – may inc 2-4 x bioavailiability • Results in exaggerated pharmacological responses and adverse effects
Assessing Function Assessing liver function is hard - no single test of how well the liver metabolises drugs Drug metabolism most likely to be impaired when the patient has cirrhosis, and has evidence of coagulation disturbances and low albumin
Pathogenetic factors(in cirrhosis) include: • alterations in intestinal absorption • alterations plasma protein binding • alterations hepatic extraction ratio • alterations liver blood flow • portal-systemic shunting • alterations biliary excretion • alterations renal clearance
Sometimes alterations increase levels of bioavailable drug, causing normal drug doses to have toxic effects • However, levels and effects for an individual drug are unpredictable and do not correlate well with the type of liver injury, its severity, or liver function test results.
Thus, no general rules are available for modifying drug dosage in patients with liver disease.
Clinical effects can vary independent of drug bioavailability, especially in chronic liver disease; eg, cerebral sensitivity to opioids and sedatives is often enhanced in patients with chronic liver disease. • Thus, seemingly small doses of these drugs given to cirrhotic patients may precipitate encephalopathy. The mechanism of this effect probably involves alterations in cerebral drug receptors
Adverse drug reactions do not appear to be more likely in patients with advanced liver disease • however, such patients may tolerate any hepatic adverse effects of drugs less well.
Learn from the mistakes of others. You can't live long enough to make them all yourself…!