Download

1 / 34
340 likes | 570 Views
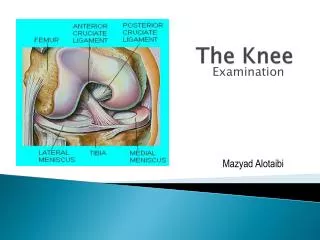
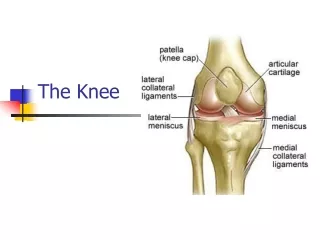
THE KNEE. KNEE ANATOMY. Bony Structures: Femur – thighbone Tibia – larger shinbone Fibula – smaller shinbone Patella: Provides anterior protection and increased leverage with knee extension. KNEE ANATOMY. Menisci: Medial and Lateral Absorbs shock Provides stability to the knee

E N D
KNEE ANATOMY • Bony Structures: • Femur – thighbone • Tibia – larger shinbone • Fibula – smaller shinbone • Patella: Provides anterior protection and increased leverage with knee extension
KNEE ANATOMY • Menisci: Medial and Lateral • Absorbs shock • Provides stability to the knee • Disperses lubrication – synovial fluid • Poor blood supply, no nerves or lymphatic channels – almost impossible to heal itself
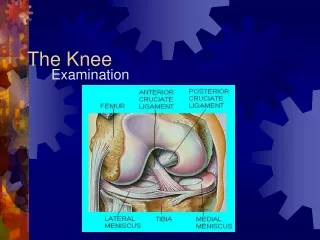
KNEE ANATOMY • Stabilizing Ligaments • Cruciate Ligaments: • ACL (Anterior Cruciate Ligament) • PCL (Posterior Cruciate Ligament) • Join the femur to the tibia in the center of the knee joint • Provides large degree of stability for the knee joint • Function: To prevent the femur and tibia from sliding and rotating away from each other
KNEE ANATOMY • Stabilizing Ligaments • Collateral Ligaments: • Medial Collateral Ligament • Lateral Collateral Ligament • Function: To prevent excessive sideways bending of the femur and tibia/fibula
ACUTE KNEE INJURIES • Include ligament strains (most common), cartilage tears, kneecap dislocations, & kneecap fractures • May be caused by a twist of the knee that forces the bones of the joint to separate (i.e. changing directions or rapidly decelerating when running) • Symptoms: Immediate pain, swelling and instability
ACL SPRAIN • ACL sprain is a stretch, tear, or complete rupture of the ligament • Cause: • A violent knee twist, usually when the foot is fixed in place (as when cleats are stuck in the ground) and the upper leg and/or body is rotated
ACL SPRAIN • Symptoms: • Immediate pain and a “pop” at the time of the injury • A sensation as if the knee is coming apart • Immediate dysfunction and instability followed by swelling • Athlete will not be able to walk without assistance
ACL SPRAIN • Athletes at Risk: • Primarily those involved in contact sports or any sport where there are rapid changes of direction when running (i.e. football, basketball, soccer, field hockey)
ACL SPRAIN • Concerns: • “The Terrible Triad” - The medial collateral ligament and medial meniscus are often injured along with the ACL
ACL SPRAIN • Recovery Time: • If surgery is required, nine to twelve months of rehabilitation is necessary before the athlete can resume vigorous activities, though it may be possible to start light running or cycling in three months.
MENISCUS INJURIES • Involves damage to one or both of the two flat, crescent-shaped pieces of cartilage that lie in the knee joint between the femur and the tibia • Medial meniscus (inner knee) is ~ five times more likely to be injured than the lateral meniscus (outer knee) • Meniscus injuries almost never heal by themselves, therefore, surgery is often required
MENISCUS INJURIES • Cause: • Excessive twisting, turning, and compression of the knee joint, possibly preceded by a single small tear that worsens over time.
MENISCUS INJURIES • Symptoms: • Onset of symptoms is usually gradual • Pain on the inner side of the knee joint during sports • Pain when pressing on the “joint line” on the inner side of the knee • Clicking or locking in the joint (caused by the torn portion of the meniscus catching on the end of the femur)
MENISCUS INJURIES • Concerns: • Left untreated, a torn meniscus may worsen to the point where the entire meniscus has to be removed instead of just repaired.
MENISCUS INJURIES • Recovery Time: • After arthroscopic surgery, the athlete can expect to return to activities that put rotational stress on the knee joint within four to eight weeks afterwards • Strengthening exercises for the muscles of the thigh should continue even after the athlete returns to sports
OVERUSE INJURIES • Include meniscus wear & tear, kneecap wear & tear, tendonitis conditions, and bursitis • Onset of symptoms is gradual • Caused by excessive sports activity, but often have an underlying risk factor • Risk factors are either internal or external
RISK FACTORS • Internal: • Usually involve deficits in strength and flexibility of the surrounding muscles, tendons, and ligaments • Also include anatomical abnormalities, such as leg length discrepancies, abnormalities in hip rotation or the position of the kneecap, bowlegs, knock-knee, or flat feet
RISK FACTORS • External: • Include training errors, improper footwear, and improper technique • Key Management of Overuse Injuries: EARLY INTERVENTION
PATELLOFEMORAL PAIN SYNDROME (PFPS) • Causes: • It is believed that most kneecap pain is caused by problems with kneecap alignment brought on by various types of anatomical abnormalities or deficits in strength and/or flexibility • This misalignment can lead to damage to the back surface of the kneecap – chondromalachia patella
PATELLOFEMORAL PAIN SYNDROME (PFPS) • Anatomical abnormalities contributing to PFPS: • Flat feet • Thighs that turn inward from the hip • Q-angle greater than 15-20 degrees • High-riding kneecaps • Shallow femoral groove • Looseness of the quadriceps tendon
PATELLOFEMORAL PAIN SYNDROME (PFPS) • Strength and flexibility deficits that may contribute to PFPS: • Weakness and/or tightness in the quadriceps, hamstrings, and calves • Weak inner quad muscle (vastus medialis) and a comparatively strong outer quad muscle (vastus lateralis) – causing the kneecap to be pulled to the outside
PATELLOFEMORAL PAIN SYNDROME (PFPS) • Symptoms: • Onset of symptoms is gradual • Usually, there is pain in front of the kneecap, and frequently, in both kneecaps • Pain may be spread out, or localized along the inner or outer edge of the kneecap • Pain intensifies during sports activity and ceases when participation stops • Usually there is no swelling, although there may be occasional puffiness in the knee
PATELLOFEMORAL PAIN SYNDROME (PFPS) • Symptoms (Cont’d): • Typically, pain develops when the person sits for extended periods with the knee bent (i.e. long car ride), as well as when walking up stairs • There may be an audible crunching, crackling in the knee • Athlete may complain of the knee “giving way”
PATELLOFEMORAL PAIN SYNDROME (PFPS) • Symptoms (Cont’d): • Symptoms usually intensify with increased sports activity levels and decrease when activity levels decline
PATELLOFEMORAL PAIN SYNDROME (PFPS) • Athletes at risk: • Primarily those engaged in sports involving excessive amounts of running/squatting • Females > Males • Concerns: • Unlikely to clear up unless true causes are identified and addressed
PATELLOFEMORAL PAIN SYNDROME (PFPS) • Recovery Time: • Both nonoperatively and after surgery, this condition takes between six to twelve weeks to resolve
PATELLAR TENDONITIS – “JUMPER’S KNEE” • Prevalent among athletes in jumping sports • An inflammation of the tendon that connects the tibia to the kneecap • One of the most common and troublesome overuse injuries in sports • Develops in three phases
PATELLAR TENDONITIS – “JUMPER’S KNEE” • Phase one (mild): Pain is felt after activity only and there is no effect on performance • Phase two (moderate): Pain is felt during and after activity. The athlete can perform at a satisfactory level. • Phase three (severe): Pain during and after activity, and it is more prolonged. Pain may be felt during daily activities. Sports performance is affected.
PATELLAR TENDONITIS – “JUMPER’S KNEE” • Causes: • Repetitive jumping – both the muscle contraction necessary for the push-off and the impact forces of the landing stress the tendon • Weak or inflexible thigh muscles predispose the athlete to this condition
PATELLAR TENDONITIS – “JUMPER’S KNEE” • Athletes at risk: • Those engaged in sports that require dynamic jumping, such as basketball and volleyball, as well as weightlifters who perform squats • Concerns: • Healing is very slow because of poor blood supply to tendons
PATELLAR TENDONITIS – “JUMPER’S KNEE” • Recovery Time • Depending on the severity, this condition can take anywhere from two weeks to several months to resolve
WHAT YOU CAN DO • Depending on the severity of the injury, it may be necessary to seek medical treatment as soon as possible