Download
1 / 40
400 likes | 600 Views
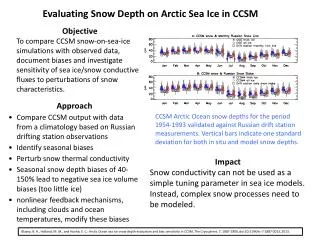
Objective Outcomes. What are they? Why do they matter?. CUSP for Mechanically Ventilated Patients October 7, 2014. Michael Klompas MD, MPH, FRCPC, FIDSA Harvard Medical School, Harvard Pilgrim Health Care Institute, and Brigham and Women’s Hospital, Boston, USA. Disclosures.

E N D
Objective Outcomes What are they? Why do they matter? CUSP for Mechanically Ventilated Patients October 7, 2014 Michael Klompas MD, MPH, FRCPC, FIDSA Harvard Medical School, Harvard Pilgrim Health Care Institute, and Brigham and Women’s Hospital, Boston, USA
Disclosures • Grant funding from the US Centers for Disease Control and Prevention • Honoraria from Premier Healthcare Alliance for lectures on VAP surveillance
Ventilator-associated pneumonia Affects ~5-10% of ventilated patients Increases ICU length of stay by ~4-7 days Increases hospital length of stay by ~14 days Crude mortality rate 30-50% Attributable mortality 8-12% Adds ~$10-50,000 to cost of hospital stay CMS 1533-P, 2007Safdar et al, Crit Care Med 2005; 33:2184Tejerina et al, J Crit Care 2006; 21:56 Muscedere et al, J Crit Care 2008;23:5-10Eber et al, Arch Intern Med 2010;170:347-353Nguile-Makao et al, Intensive Care Med 2010;36:781-9Beyersmannet al, Infect Control HospEpidemiol2006;27:493
Diagnostic Criteria for VAP Ego et al. Chest 2014;ePub ahead of print
Impact of Diagnostic Criteria on VAP Prevalence Prospective surveillance, 1824 patients, Tertiary Med-Surg Unit, Belgium Ego et al. Chest 2014;ePub ahead of print
All VAP Signs Subjective, Non-Specific, or Both The core clinical signs associated with VAP: Radiographic opacities Fever Abnormal white blood cell count Impaired oxygenation Increased pulmonary secretions
Interobserveragreement in VAP surveillance 50 ventilated patients with respiratory deterioration IP 2(20 VAPs) IP 1 (11 VAPs) 3 7 1 7 3 0 5 IP 3 (15 VAPs) Kappa = 0.40 Klompas, AJIC 2010:38:237
6 Case Vignettes Presented to 43 Surveyors Crit Care Med 2014;42:497
Accuracy of clinical diagnosis of VAPRelative to 253 autopsies • Loose definition: • Infiltrate and 2 of • temp / wbc / purulence 100% 80% Sensitivity / Positive Predictive Value 60% • Strict definition: • Infiltrate and 3 of • temp / wbc / purulence 40% 20% 0% Sensitivity PositivePredictiveValue Tejerina et al., J Critical Care 2010;25:62
Accuracy of quantitative BAL culturesRelative to histology 100% 80% Sensitivity / Positive Predictive Value 60% 40% 20% 0% Sensitivity PositivePredictiveValue Kirtland, Chest 1997;112:445Fabregas, Thorax 1999;54:867Chastre, Am Rev RespirDis 1984;130:924Torres, Am J RespCrit Care Med1994;149:324Marquette, Am J RespCrit Care Med 1995;151:1878Papazian, Am J RespCrit Care Med 1995;152:1982
The VAP Prevention Paradox Crit Care 2009;13:315
Reasons for the Prevention Paradox VAP diagnosis is subjective The case of chlorhexidine VAP diagnosis is non-specific The case of silver-coated ETTs Many VAP studies under-powered The case of head of bed elevation
Reasons for the Prevention Paradox VAP diagnosis is subjective The case of chlorhexidine VAP diagnosis is non-specific The case of silver-coated ETTs Many VAP studies under-powered The case of head of bed elevation
Oral CHG in Non-Cardiac Surgery Patients Open Label Studies: RR 0.61 (0.35-1.04) Double-Blind Studies: RR 0.88 (0.66-1.16) JAMA Internal Med 2014;174:751
Routine Oral Care with Chlorhexidine • Impact on mean duration of mechanical ventilation: • NONE • Impact on ICU length-of-stay • NONE • Impact on mortality • POSSIBLE INCREASE!!! RR 1.13 (0.99 to 1.28) JAMA Internal Med 2014;174:751
Reasons for the Prevention Paradox VAP diagnosis is subjective The case of chlorhexidine VAP diagnosis is non-specific The case of silver-coated ETTs Many VAP studies under-powered The case of head of bed elevation
Silver-Coated Endotracheal TubesVAP Rates and Outcomes Conventional ETTs Silver coated ETTs 12.0 6.0 5.0 10.0 4.0 8.0 VAPs per 100 Patients Lengths of Stay (days) 6.0 3.0 2.0 4.0 1.0 2.0 0 0 Hospitaldays ICUdays Ventdays VAP Incidence JAMA 2008;300:805
Silver-coated endotracheal tubesMicrobiological Outcomes VAP Counts Included: yeast, normal flora, coag-negStaph, & Enterococcus
Reasons for the Prevention Paradox VAP diagnosis is subjective The case of chlorhexidine VAP diagnosis is non-specific The case of silver-coated ETTs Many VAP studies under-powered The case of head of bed elevation
N=86 78% in VAP, P=.04 N=221 71% in VAP, P>.10 Reducing the risk of ventilator-acquired pneumonia through head of bed elevation Nursing Crit Care 2007;12:287 46% in VAP, P>.10 N=30
Semi-recumbent position and ICU Days Difference in ICU Length of Stay Drakulovic, Lancet 1999 (difference in means) van Nieuwenhoven, CCM 2006 (difference in medians) Keeley, Nursing Crit Care 2007 (not reported) ??? All studies +2 +1 0 -2 -1 Favors Semi-Recumbent Position Favors Supine Position
Ventilator-associated conditions (VAC) Rise in daily minimum PEEP ≥3cm or FiO2 ≥20 sustained ≥2 days after ≥2 days of stable or improving daily minimum PEEP or FiO2 VAC
Impact of VAEs on length-of-stayControlled for time to VAE, age, sex, unit, comorbidities, severity of illness. All comparisons are to patients without VAE (control). Control VAC *** IVAC *** Possible VAP *** Probable VAP *** Control VAC *** IVAC *** Possible VAP *** Probable VAP *** Days Infect Control HospEpidemiol2014;5:502-510
Impact of VAEs on mortality VAE VAP 0.5 1 2 5 10 Odds Ratio or Hazard Ratio
Canadian Critical Care Trials Group ABATE StudyEnhanced care for vented patients, 11 ICUs, 1330 patients Muscedere et al. Chest 2013;144:1453-1460
Conservative Fluid Management • 304 patients randomized to daily BNP levels versus usual care • Patients randomized to daily BNP levels • More diuretics, negative fluid balance • Less time to extubation • 50% fewer VAEs P=.02 Dessap et al. Chest 2014; ePub ahead of print
The VAP Prevention Paradox Crit Care 2009;13:315
The Upshot • VAP rates are unreliable outcomes • VAE rates likely reliable but still very new. Unclear how best practices will impact them. • If we want to know whether a prevention measure really works or not, we have to look at objective outcomes such as: • duration of mechanical ventilation • ICU length-of-stay • hospital length-of-stay • mortality
Minimize sedation Greater sedation associated with longer ventilator and ICU stays. Increases risk for pneumonia and other infections. RCT data from Denmark showing that vented patients can be adequately managed with NO sedation Spontaneous awakening trials associated with less overall sedative use and earlier extubation http://ppcdrugs.com/en/products/alphabetical/midazolam-1mg-5ml/ NEJM 1996;335:1864-9 NEJM 2000;342:1471-7 Lancet 2008;371:126-134 Lancet 2010;375:475-80
Paired daily sedative interruptions and spontaneous breathing trials Wake Up and Breathe • Spontaneous breathing trials associated with earlier extubation • Patients are more likely to pass spontaneous breathing trials if they’re awake for the trial • RCT data showing that pairing SATs with SBTs speeds extubation by ~3 days and shortens ICU and hospital LOS by ~4 days compared to SBTs alone Lancet 2008;371:126-134 NEJM1996;335:1864-9
Early mobility – Wake Up & Walk! • Early mobilization assocaited with less time to extubation and shorter ICU stays • May also help prevent atelectasis & delirium • As with improved sedative management and weaning protocols, less time on vent means less time at risk for VAEs Lord et al., Crit Care Med 2013;41:717 Schweickert et al., Lancet 2009;373:1874 Needham et al., Arch Phys Med Rehabil2010;91:536 http://69.36.35.38/images/CHESTPhysician/CritCareCom0610Fig2.jpg
Low tidal volume ventilation • Higher tidal volumes associated with acute lung injury • Randomized controlled trial data showing that lower tidal volumes protect against acute lung injury in patients without ARDS and lower mortality rates in patients with ARDS http://page2anesthesiology.org/2012/less-rather-than-more-volume-is-better-when-ventilating-patients-after-cardiac-surgery/ Determann, Critical care2010;14(1):R1 ARDSnet, NEJM 2000;342:1301-1308
Summary • VAP diagnosis is subjective and non-specific • Inconsistent association between VAP and patient outcomes • Many interventions purportedly lower VAP rates but no impact on patient outcomes: “the VAP Prevention Paradox”. • Makes VAP an unreliable outcome • VAEs more objective and consistently predict adverse outcomes… but the definitions are still very new, very little data so far on how prevention strategies impact VAE rates • Implication: need to look at objective outcomes if we want to be sure that CUSP 4 MVP is helping our patients
Michael Klompas (mklompas@partners.org) Thank you!
Am J RespCrit Care Med 2014;8:947 Chest 2014;ePub ahead of print