Download
1 / 47
470 likes | 486 Views
Surgical Fires: Prevention & Management. Debnath Chatterjee, MD, FAAP Children’s Hospital Colorado University of Colorado. Disclosure. Nothing to disclose. Learning Objectives. Identify components of the surgical fire triangle Explain the risks of an oxygen-enriched atmosphere

E N D
Surgical Fires:Prevention & Management Debnath Chatterjee, MD, FAAP Children’s Hospital Colorado University of Colorado
Disclosure • Nothing to disclose
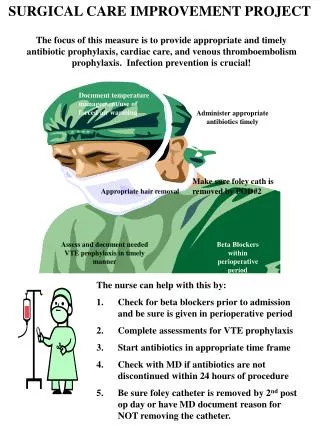
Learning Objectives • Identify components of the surgical fire triangle • Explain the risks of an oxygen-enriched atmosphere • Describe strategies for the prevention of surgical fires • Perform a preoperative surgical fire risk assessment • Discuss appropriate steps in the management of surgical fires
Outline • Overview of surgical fires • High risk procedures • Components of the surgical fire triangle • Preoperative fire risk assessment • Prevention of surgical fires • Management of surgical fires
Surgical Fires • Fires that occur in, on or around a patient while undergoing a surgical or medical procedure • ~ 550-650 surgical fires occur in US every year1 • Pennsylvania Patient Safety Advisory2 • 1/3rd of reported events indicated harm to patient 1. Health Devices 2009 Oct;38 (10):314-332 2. Clarke JR, Bruley ME. Pa Patient Safety Advis 2012
Surgical Fires • Equipment involved • 70%- Electrosurgical device • 10%- Laser • Other- Fiberoptic light source, defibrillator, high speed burrs • Oxidizer and fuels • 75% - Oxygen enriched atmosphere • 4% - Alcohol based prep solutions Health Devices 2009 Oct;38 (10):314-332
Location of Surgical Fires Health Devices 2009 Oct;38 (10):314-332 Reprinted with permission from ECRI Institute
High Risk Procedures When ignition source can come in proximity to an oxidizer- enriched atmosphere • Tonsillectomy • Tracheostomy • Removal of laryngeal papillomas • Cataract/other eye surgery • Burr hole surgery • Removal of lesions on head, neck or face ASA Practice Advisory for the Prevention & Management of OR Fires. Anesthesiology 2013; 118 (2): 271-90
Initiatives to Prevent Surgical Fires Joint Commission Sentinel Event Alert 2003 ASA Practice Advisory 2008 FDA Initiative 2011 Joint Commission National Patient Safety Goal 2006-2009 APSF Fire Safety Video 2010
Initiatives to Prevent Surgical Fires Anesthesiology 2013; 118(2): 271-290. Anesthesia Patient Safety Foundation Fire Safety video www.apsf.org/resources/fire-safety/ FDA Initiative www.fda.gov/Drugs/DrugSafety/SafeUseInitiative/PreventingSurgicalFires
Surgical Fire Triangle Reprinted with permission from ECRI Institute
Controlling Oxidizers • Oxidizers support combustion • Include oxygen, nitrous oxide and air Oxygen enriched atmospheres (OEA) • involved in majority of surgical fires • when O2 concentration exceed 21% by volume • lowers temperature and energy at which a fuel will ignite Health Devices 2009 Oct;38 (10):314-332
Oxygen Enriched Atmosphere • OEA fires are • hotter • more vigorous • spread more rapidly Health Devices 2009 Oct;38 (10):314-332 Reprinted with permission from ECR Institute
Oxygen Enriched Atmosphere • Configuration of surgical drapes + open delivery of O2 can result in O2 build up, increasing the risk of fires Reprinted with permission from ECRI Institute
Flammability of Surgical Materials in Varying Concentrations of Oxygen Time to ignite and total burn time decreased as O2 concentration increased (P < 0.001) Culp WC et al. Anesthesiology 2013: 119 (4) 5 surgical materials were ignited in 3 O2 concentrations
Controlling Oxidizer Nitrous Oxide • Supports combustion • Fires involving O2/N2O mixtures can be as easily ignited and as severe as fires involving 100% O2
Controlling Oxidizers Ambient Air • 21% oxygen/78% Nitrogen • Supports combustion Medical Air • Supports combustion • Not O2 enriched at ambient pressure when delivered to patient Health Devices 2009 Oct;38 (10):314-332
During Head, Neck, Face and Upper Chest Surgery: Can patient maintain safe SpO2 without supplemental O2? Yes No Use air for open delivery Secure airway with LMA or ETT Health Devices 2009 Oct;38 (10):319
When is it OK to Use Open O2 Delivery on Face? • Certain procedures require verbal responses from patient intraoperatively • Carotid artery surgery • Neurosurgery • Pacemaker insertion Health Devices 2009 Oct;38 (10):319
Prevention Strategies During Open O2 Delivery • Deliver minimum O2 concentration necessary for adequate oxygenaton • Begin with 30% FiO2 and increase up if necessary • If using > 30% FiO2, deliver 5-10 L/min of air under drapes to wash out excess O2 • Stop supplemental O2 at least one minute before and during use of electro surgery unit (ESU) or laser Health Devices 2009 Oct;38 (10):319
Options for Blending Air and O2 for Open Delivery • Use an independent O2-air blender • Use blended gas from common gas outlet (CGO) on anesthesia machine • For anesthesia machines that don’t have a CGO, use breathing circuit to deliver blended gas Health Devices 2009 Oct;38 (10):314-332 Reprinted with permission from Silverstein, KL.
Ignition Sources • Electrosurgical units -most common • Surgical laser- 2nd most common • Electrocautery (hot wire) devices • Fiberoptic light source • Defibrillators • High speed burrs Health Devices 2009 Oct;38 (10):314-332
When Using Electrosurgery, Electrocautery or Laser: • Notify surgeon of the presence of, or an increase in oxidizer-enriched atmosphere • Activate unit only when the active tip is in view Deactivate unit before the tip leaves the surgical site • Place unit in a holster when not in active use • Place lasers in standby mode when not in active use • Do not place rubber catheter sleeves over electrosurgical electrodes Health Devices 2009 Oct;38 (10):319
Fuels in the OR * Betadine skin prep is not flammable Health Devices 2009 Oct;38 (10):314-332
Fuels in the OR Health Devices 2009 Oct;38 (10):314-332
Managing Fuels • Be aware that alcohol-based preps are flammable • Avoid pooling, spilling or wicking of flammable preps • Allow flammable liquid preps to dry fully before draping- 3 min • Remove towels used to catch dripped flammable prep before draping • Moisten sponges when used in proximity to ignition source Health Devices 2009 Oct;38 (10):314-332
Prevention Strategies During Open O2 Delivery on Face • Use an adherent incise drape, to help isolate the incision from possible O2 enriched atmosphere • Keep fenestration towel edges as far from the incision as possible • Arrange drapes to minimize O2 buildup underneath • Coat head hair and facial hair with water soluble lubricating jelly to make it nonflammable Health Devices 2009 Oct;38 (10):314-332
Reprinted with permission from ASA Practice Advisory for the Prevention & Management of OR Fires. Anesthesiology 2013
NEW APSF Prevention Algorithm 2012 Anesthesia Patient Safety Foundation. Surgical fire injuries continue to occur: Prevention may require more cautious use of oxygen. APSF Newsletter Winter 2012;26(3):42-43
Fire Risk Assessment • Should be included in ‘Surgical Time Out’ to identify and assess fire risks • Enables a discussion among all team members on: • Identifying elements of surgical fire triangle pertinent to case • Assessing the risk of a surgical fire • Developing strategies for the prevention of a surgical fire • Designating roles for each team member in the event of a surgical fire
Silverstein Fire Risk Assessment Tool Link to Christiana Care Health System Surgical Fire Risk Assessment Tool: www.christianacare.org/FireRiskAssessment (Accessed 12/23/13) Reprinted with permission from Silverstein, KL.
Silverstein Fire Risk Assessment Tool Reprinted with permission from Silverstein KL, Christiana Care Health Systems, Newark, DE
Preventing Airway Fires While using electrosurgery units (ESU) • Do not use ESU to cut into the trachea • If long, insulated ESU probes are needed to prevent mouth burns (e.g. tonsillectomy): • Use only commercially available insulated probes • Do not use red rubber catheters to sheathe probes
Preventing Airway Fires While using electrosurgery units (ESU) • When operating in oropharynx, • Scavenge deep with a metal suction cannula to catch leaking O2 and N2O • Use moistened sponges
Preventing Airway Fires While using laser: • Limit laser output to the lowest clinically acceptable power density and pulse duration • Place laser in standby mode when not in use • Activate laser only when the active tip is in view • Consider using laser resistant tracheal tube during upper airway surgery, if appropriate • Use saline in cuff to prevent cuff ignition • Use dye in cuff to indicate puncture
Management of Surgical Fires Recognizing early signs of a surgical fire • Unusual sounds (“pop, snap or foomp”) or odors • Unexpected smoke/heat • Unexpected movement of drapes • Discoloration of drapes or breathing circuit • Unexpected patient movement or complaint • Unexpected flash or flame ASA Practice Advisory for the Prevention & Management of OR Fires. Anesthesiology 2013; 118 (2): 271-90
Airway Fire For a fire in the airway or breathing circuit, ASAP: • Remove the tracheal tube • Stop the flow of all airway gases • Disconnect breathing circuit • Remove all flammable and burning materials from airway • Pour saline or water into the patient’s airway Perform rapidly & simultaneously ASA Practice Advisory for the Prevention & Management of OR Fires. Anesthesiology 2013; 118 (2): 271-90
Airway Fire If the airway or breathing circuit fire is extinguished: • Reestablish ventilation by mask • Avoid supplemental O2& N2O, if possible • Extinguish and examine ETT to assess for fragments • Consider rigid bronchoscopy to assess injury & remove debris ASA Practice Advisory for the Prevention & Management of OR Fires. Anesthesiology 2013; 118 (2): 271-90
Non Airway Fire For a fire elsewhere on or in the patient, immediately • Stop the flow of all airway gases • Remove all drapes, flammable and burning material from the patient • Extinguish all burning materials in, on or around the patient with saline or water • Assess for smoke inhalation injury if patient not intubated ASA Practice Advisory for the Prevention & Management of OR Fires. Anesthesiology 2013; 118 (2): 271-90
Extinguishing: Pat out if very small. Reprinted with permission from ECRI Institute
Extinguishing: Rip off! Reprinted with permission from ECRI Institute
Reprinted with permission from ASA Practice Advisory for the Prevention & Management of OR Fires. Anesthesiology 2013; 118 (2): 271-90
Extinguishers: Rarely Needed in OR For placement in each OR and use on patient: CO2 Extinguisher Not:* Water, dry chemical, water mist, or fire blanket *For published rationale for not using these in the OR see: www.ecri.org/surgical_fires Reprinted with permission from ECRI Institute
If Evacuation is Necessary Health Devices 2009 Oct;38 (10):314-332
Summary • Surgical fires are preventable • Fire safety in the OR is every member’s responsibility and requires a team approach • Minimizing or eliminating enriched oxygen delivery is fundamental • Comprehensive fire safety program is critical
References • New Clinical Guide to Surgical Fire Prevention. Health Devices 2009 Oct;38(10): 314-32 • Clarke JR, Bruley ME. Surgical Fires: Trends associated with prevention efforts. Pennsylvania Patient Safety Advisory 2012 Dec;9(4):130-5 • Apfelbaum JL et al. Practice Advisory for the Prevention and Management of Operating Room Fires. Anesthesiology 2013;118(2): 271-90 • Culp WC, Kimbrough BA, Luna S. Flammability of surgical drapes and materials in varying concentrations of oxygen. Anesthesiology 2013;119(4): 770-6