Download
1 / 29
290 likes | 436 Views
Aneurysms; The Bubble Burst. Mr JV Smyth Vascular Surgery. ‘Atherosclerotic’ Mycotic Inflammatory Connective tissue disorder False. Simple Ureteric compression AV fistula Aortoenteric fistula Rupture Thrombosis/Embolism. Aortic/iliac Popliteal Visceral Intracerebral. Asymptomatic

E N D
Aneurysms; The Bubble Burst Mr JV Smyth Vascular Surgery
‘Atherosclerotic’ Mycotic Inflammatory Connective tissue disorder False Simple Ureteric compression AV fistula Aortoenteric fistula Rupture Thrombosis/Embolism Aortic/iliac Popliteal Visceral Intracerebral Asymptomatic Back pain Tenderness Limb ischaemia Threshold for surgery Fusiform Saccular
The Paradigm Abdominal aortic aneurysm Asymptomatic Atherosclerosis Fusiform Infrarenal Principal risk is rupture
Aneurysms • Males 4:1 • 60’s and upward • Hypertensive smokers • Family history of AAA • 1 in 25 random 65yr males • 1 in 6 65 yr HT male smokers with FH • Usually incidental finding during Ix for something else
SCREENING • Common condition • Significant outcome if not diagnosed • Effective intervention • At-risk population subgroup • Widely available test • Safe, sensitive and specific • Economic (QALY) • National AAA screening programme recently announced
Open repair • Replace aneurysmal segment • GA, laparotomy, aortic XC • Mortality 5-7% • 90% cardiac • Occasional respiratory/renal failure/PE • Patient selection • Echo, stress test • PFTs
Maximum transverse diameter Normal aorta < 2.5cm Ectasia < 3.5cm Small AAA < 4.5cm Large AAA >5.5cm Rupture is exponentially associated with MTD ~1% Annual risk at 4cm ~ 7% Annual risk at 6cm ~30% annual risk at 8cm
Endovascular repair • Reline aorta rather than replace • Dependent on radial force of stents for fixation rather than sutures • Modular system • Bilateral groin incisions (or punctures) • Avoids laparotomy, XC • Mortality 1.9% (EVAR 1 trial)
Why not everyone ? EARLY ENDOLEAKS
Endoleak Types • I around aortic or iliac landing zones • II from lumbars or IMA • III between graft components • IV loss of graft integrity
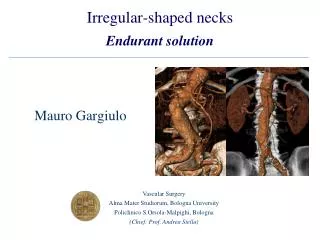
Anatomical suitability • Infrarenal neck, common iliac arteries • Length • Shape • Angulation • Thrombus • Iliac access • Tortuosity • Calibre
Oversizing • Suprarenal uncovered stent • Barbs • More flexible devices • Repositioning capability • Low profile delivery system • Custom made prosthesis
Complex EVAR • Iliac conduit • Carotid access • Iliac bifurcation device • Aorto-uniiliac and cross over • IIA embolisation • Fenestrated • Branched • Chimney
Why not everyone ? LATE ENDOLEAKS
Long term FU • Device integrity • Conformational change • Reinterventions proportional to time
Ruptured AAA • Lower back pain, hypotension, abdo mass • Most never get to hospital • Overall mortality 95% • Postoperative mortality ~50% • Get large IV lines in • Call vascular surgeons • Permissive hypotension, analgesia • Send blood for XM, FBC, clotting, U&E