Download
1 / 57
570 likes | 917 Views
SOLUBLE FIBRIN. MONKEY (E. COLI INJECTION). HUMAN (ACUTE LEUKEMIA). CAUSES OF DIC. Blood exposed to excess tissue factor Endothelial damage Tissue factor expression by monocytes Massive tissue/organ injury Cancer Obstetric catastrophe Activation of fibrinolysis

E N D
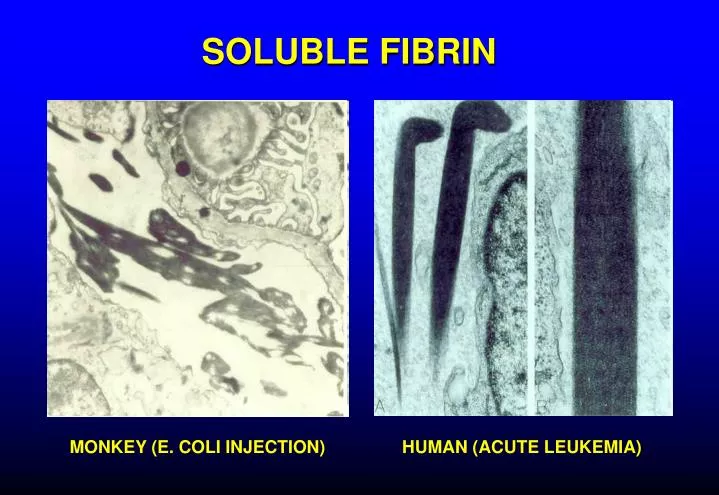
SOLUBLE FIBRIN MONKEY (E. COLI INJECTION) HUMAN (ACUTE LEUKEMIA)
CAUSES OF DIC Blood exposed to excess tissue factor Endothelial damage Tissue factor expression by monocytes Massive tissue/organ injury Cancer Obstetric catastrophe Activation of fibrinolysis Secondary to thrombin formation (t-PA) Cancer/leukemia (t-PA, u-PA, other) Cardiopulmonary bypass Other procoagulant or profibrinolytic substances Cancer cells Venoms
TFPI TFPI AT3 APC TFPI AT3 AT3 APC F. VIII/F. IX APC F. VII Tissue factor Thrombin PL, Ca++ TFPI APC F. II F. X/F. V AT3 AT3 TFPI APC APC AT3 TFPI
Thrombin Tissue factor F. VIII/F. IX F. VII Tissue factor Thrombin PL, Ca++ F. II F. X/F. V Tissue factor Thrombin
TISSUE FACTOR Ubiquitous lipoprotein Highest concentrations in mucosa, brain, skin, vascular adventitia "hemostatic envelope" Not normally expressed by endothelium or circulating cells Expression induced by inflammatory cytokines Major physiologic (and pathologic) initiator of coagulation
MONOCYTE + ENDOTOXIN SMALL VESSEL LARGE VESSEL MONOCYTE TISSUE FACTOR Am J Pathol 1989; 134:1087-97
Control 5 nM TNF x 90 min 5 nM TNF x 24h CYTOKINE-INDUCED GAPS IN ENDOTHELIAL MONOLAYER J Exp Med 1989;169:1977-91
KINETICS OF MONOCYTE TISSUE FACTOR mRNA EXPRESSION AND THROMBIN GENERATION AFTER ADMINISTRATION OF BACTERIAL LIPOPOLYSACCHARIDE TO HEALTHY VOLUNTEERS Tissue factor mRNA Thrombin Franco et al, Blood 2000;96:554-9
Cancer cells shed procoagulant membrane vesicles Fibrin deposits around tumor cells Intravascular fibrin Dvorak et al, 1981
SECRETED PRODUCTS OF MYELOBLASTS Urokinase Tissue factor tPA Elastase Cytokines
PROMOTERS OF DIC Inflammation (TNF, IL-1, IL-6, etc) Upregulation of procoagulant pathways Downregulation of profibrinolytic pathways Effects on endothelium Liver disease Inhibitor deficiency (antithrombin, antiplasmin, protein C, etc) Diminished clotting factor production Delayed clearance of FDP
TNF IL-1 IL-3/IL-6 monocyte endothelial liver megakaryocyte cell Tissue factor expression Decreased Thrombomodulin Increased PAI-1 Increased Platelets Increased Fibrinogen, antiplasmin INFLAMMATORY CYTOKINES
Fibrin deposition in kidney in DIC induced by tissue factor (TF) or bacterial lipopolysaccharide (LPS) in rats Asakura et al, Crit Care Med 2002;30:161
RELATIONSHIP BETWEEN MORTALITY AND TNF LEVEL IN CHILDREN WITH INFECTIOUS PURPURA FULMINANS 100 80 Under 0.15 0.15-0.50 60 0.50-1.00 Mortality (%) 40 Over 1.00 20 0 TNF level (ng/ml) NEJM 1988;319:397-400
COMPLICATIONS OF DIC Bleeding Thrombosis Tissue necrosis
CAUSES OF BLEEDING IN DIC Clotting factor consumption High levels of FDP (inhibit fibrin formation) Endothelial damage Increased fibrinolytic activity
FIBRINOLYSIS Platelets Plasminogen Endothelial cell Fibroblasts PAI-1 TPA UK Macrophage Plasmin Liver PI PI 2 2 Fibrin FDP Fibrinogen
Bleeding severity vs antiplasmin activity patients with platelets > 30,000 100 80 0-2+ bleeding 60 % of patients 3-4+ bleeding 40 20 0 < 50% 50-75% > 75% Antiplasmin activity
Examples DIC WITH HYPERFIBRINOLYSIS Acute leukemia (particularly promyelocytic) Metastatic cancer (esp. prostate) Cardiopulmonary bypass Liver disease or transplantation
THROMBOSIS IN DIC Large vessel thrombosis uncommon Disordered clotting Increased fibrinolysis More common in "chronic DIC" e.g., Trousseau syndrome Clots may form around intravascular catheters, etc
TISSUE NECROSIS AND DIC (PURPURA FULMINANS) Contributing factors Intravascular fibrin Endothelial damage Downregulated fibrinolysis Hypotension Pressor administration Acquired protein C deficiency
PUPURA FULMINANS Pneumococcal sepsis in splenectomized patient High level bacteremia NEJM 2001;344:1593 NEJM 2004;351:2636
PURPURA FULMINANS IN MENINGOCOCCEMIA High level bacteremia Blood 2005;105:11 NEJM 2001;344:1372
TISSUE NECROSIS IN PURPURA FULMINANS ADRENAL GLAND (Waterhouse-Friderichsen syndrome) NEJM 2005;353:1245 RENAL CORTEX Hum Pathol 1972;3:327
PROTEIN C Physiologic anticoagulant Vitamin K-dependent Destroys factors Va, VIIIa (Protein S is cofactor) Activated by thrombin bound to endothelium Activation downregulated by inflammatory cytokines Protective effect on endothelium? Protein C receptor on endothelial cells Activated protein C modulates endothelial response to inflammation and hypoxia Severe deficiency of protein C can cause tissue necrosis
THE PROTEIN C SYSTEM Blood 2007; 109:3161
CYTOPROTECTION BY APC Blood 2007; 109:3161
PROTEIN C OR S DEFICIENCY STATES ASSOCIATED WITH THROMBOSIS OR PURPURA FULMINANS Situation Mechanism Clinical Manifestations Inherited protein C or S deficiency (homozygous) Neonatal purpura fulminans Genetic Inherited protein C or S deficiency (heterozygous) Increased risk of venous thromboembolism Genetic Heterozygous protein C (or S?) deficiency + warfarin Rx Genetic + decreased protein C synthesis Warfarin-induced skin necrosis ? Immune-mediated protein S consumption Post-infectious purpura fulminans Varicella infection ? Protein C and S consumption (DIC) or downregulation Meningococcemia Meningococcal purpura Acquired protein C inhibitor ? Monoclonal Ig binds protein C or APC Purpura fulminans
HOMOZYGOUS PROTEIN C DEFICIENCY WITH NEONATAL PURPURA FULMINANS
Baboon model PROTEIN C IN BACTERIAL SEPSIS With normally lethal dose of E. coli: Activated protein C prevents DIC, tissue necrosis and death Another inhibitor of thrombin formation blocks DIC but not tissue necrosis and death With normally sublethal dose of E. coli: Monoclonal antibodies to either protein C or its endothelial receptor promote DIC, tissue necrosis and death F.B. Taylor et al, J Clin Invest 1987; Blood 1991; Blood 2000
TRANSGENIC MICE THAT OVEREXPRESS THE ENDOTHELIAL APC RECEPTOR HAVE IMPROVED SURVIVAL AFTER ENDOTOXIN ADMINISTRATION J Thrombos Haemost 2005;3: 1351–1359
CIRCULATING ACTIVATED PROTEIN C IN SEVERE SEPSIS Survivors had higher APC levels and lower F1.2/APC ratios than non-survivors Blood 2004;104:3958
ENDOTHELIAL PROTEIN C ACTIVATION IS REDUCED IN SEPSIS Normal Sepsis Thrombomodulin Protein C receptor NEJM 2001;345:408
ANTICOAGULANT PROTEIN LEVELS IN MENINGOCOCCEMIA Relationship to multiorgan failure Mean level (% normal) ORGAN FAILURE? Protein C Antithrombin Protein S Yes 18 ± 7 53 ± 16 75 ± 19 No 42 ± 13 81 ± 20 87 ± 14 Blood 2000;96:3719
Protein C levels predict ICU survival as well as the APACHE II or SAPS II score Anesthesiology 2007;107:15
Summary DIC PATHOPHYSIOLOGY Excess tissue factor + flowing blood = DIC Inflammatory cytokines set the stage for DIC and contribute to tissue damage Excessive fibrinolysis associated with higher bleeding risk Acquired protein C deficiency associated with high risk of tissue necrosis/purpura fulminans
DIAGNOSIS OF DIC DIC is likely when there is A condition known to cause DIC Evidence of accelerated fibrinolysis and clotting factor consumption
LABORATORY TESTS IN DIC ASSESS SEVERITY GUIDE TREATMENT DIAGNOSIS FDP or D-Dimer Antithrombin III PT/INR Fibrinogen Fibrinogen Alpha2-antiplasmin PT/INR Platelet count Protein C Platelet count Alpha2-antiplasmin Fibrin monomer
Death Is Coming
OUTCOME IN DIC • 346 patients • Incidence of bleeding: 77% • Mortality • Overall: 68% • With bleeding: 72% • Without bleeding: 63% • Most deaths from underlying disease, not bleeding Thromb Haemost 1980; 43:28-33
TREATMENT OF DIC TREAT UNDERLYING DISEASE! Clotting factor & inhibitor replacement Fresh frozen plasma Cryoprecipitate Platelets ?Antithrombin III, protein C concentrate Pharmacologic inhibitors Heparin Antifibrinolytics
REPLACEMENT THERAPY IN DIC Product Content Indication Risk Volume, virus transmission All clotting factors and inhibitors FFP INR > 1.6 Fibrinogen, VIII, VWF Fibrinogen < 50-100 (?) Cryoprecipitate "Feed the fire"? Platelets Platelets < 30-50K Purified antithrombin Antithrombin Low antithrombin? ? Purpura fulminans? Low protein C? Activated protein C Purified APC Bleeding
PHARMACOLOGIC INHIBITORS IN DIC Anticoagulant: UnfractionatedHeparin Little experience with LMWHs Antifibrinolytic: Epsilon aminocaproic acid (Amicar) Tranexamicacid (?availability) No controlled trials showing benefit Convincing anecdotal evidence of benefit in individual patients
HEPARIN IN DIC Rationale: Prevent thrombin/fibrin formation and secondary fibrinolysis Indications: Cancer-associated DIC Acute leukemia and DIC Chronic DIC with aneurysm, etc Overt thrombosis Purpura fulminans? Concomitant antifibrinolytic Rx Risks: Exacerbate bleeding Drug-induced thrombocytopenia Low dose (eg, 500 U/hr) usually adequate
H N 2 H N CH CH CH CH CH COOH LYSINE 2 2 2 2 2 H N CH CH CH CH CH COOH AMICAR 2 2 2 2 2 2 (EACA) CH CH 2 2 TRANEXAMIC CH CH COOH H N CH 2 2 ACID CH CH 2 2 ANTIFIBRINOLYTIC DRUGS
FIBRINOLYSIS Antifibrinolytic drug effects Plasminogen EACA TPA UK EACA Plasmin EACA Fibrin FDP Fibrinogen
ANTIFIBRINOLYTIC THERAPY IN DIC Rationale: Inhibit activation of plasminogen/clot lysis Prevent bleeding Indications: DIC in promyelocytic leukemia DIC with severe bleeding, low antiplasmin? Risk: Thrombosis Amicar, 1 gram/hour i.v. with low dose heparin
SPINAL ARTERY THROMBOSIS AFTER AMICAR TREATMENT Hum Pathol 1972;3:327