Download
1 / 53
580 likes | 1.26k Views
Testicular Seminoma. The Nuts and Bolts of Therapy Matthew Harkenrider, MD Radiation Oncology PGY4. Epidemiology. Accounts for only 1-2% of all cancers in men, but… The most common solid tumor in males between 15 and 35 years of age Estimated 8450 new cases, 350 deaths in US in 2010

E N D
Testicular Seminoma The Nuts and Bolts of Therapy Matthew Harkenrider, MD Radiation Oncology PGY4
Epidemiology • Accounts for only 1-2% of all cancers in men, but… • The most common solid tumor in males between 15 and 35 years of age • Estimated 8450 new cases, 350 deaths in US in 2010 • Cumulative lifetime risk for a white American male is 0.2% • Seminoma seen more frequently in 25-45 yrs, NSGCT seen more in 15-30 year age group
Etiology • Environmental factors? • Mumps orchitis, immunosuppression following organ transplant, HIV • History of trauma likely leads to testis examination leading to finding unrelated testicular cancers • Prenatal factors including threated miscarriage, excess maternal nausea, C-section • The only definitely associated factors are…
Etiology • Cryptorchidism (undescended testicle) • 5x increased risk (1 in 100) • Orchipexy before puberty lowers risk some • 5-20% occur in contralateral testicle • Mechanism unknown – temperature? trauma? • Previous testicular cancer • Seminoma – 3.6% @ 25 years • Non-seminoma – 8.4% @ 25
Prevention and Early Detection • Screening? • No formal screening recommended • Most found on self exam or by chance • Pt’s with previous h/o Testicular CA should have routine examination
Clinical Evaluation • Most common presentation is a painless testicular mass. About 45% will have some pain • After a mass is detected… • Testicular U/S – shows solid mass • Tumor Markers • AFP is elevated in NSGCT (or mixed with NSGC component), but not in seminoma • β-hCG found in NSGCT and 5-10% of seminoma • LDH 30-80% of seminoma • Radical Inguinal Orchiectomy – tumor staging • CT Abd/Pelvis – nodal staging • CXR – metastatic staging
Pathology • The vast majority (>95%) of testicular cancers are GCT’s • Classified into seminomatous and nonseminomatous for clinical purposes • 60% pure seminoma, 30% NSGCT, 10% mixed • A characteristic chromosome abnormality in GCTs of all histologic types is the 12p isochromosome
Pathology – Seminoma • Well demarcated from normal tissue • Virtually all express placental leukocyte alkaline phospatase (PLAP) • Anaplastic seminoma when >3 mitosis/hpf which is a more aggressive variant
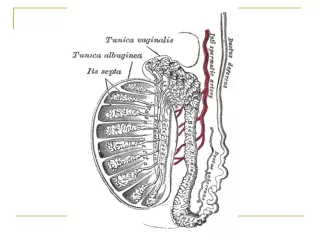
Pathways of Spread • Local extension occurs • into epididymis (T1) • Through tunica vaginalis (T2) • Into spermatic cord (T3) • Into scrotum (T4)
Pathways of Spread • Lymphatic spread • Right testis interaortocaval precaval paraaortic • Left testis paraaortic preaortic interaortocaval • Contralateral involvement found in approx 15% • Pelvic and inguinal involvement occurs in <3% • Supradiaphragmatic involvement can occur via the thoracic duct • Supraclavicular involvement can occur in the setting of relapse
Nodal Staging • N0 – negative • N1 – ≤ 2 cm • N2 – 2.1-5.0 cm • N3 – >5 cm
Staging • Stage I – any T, N0, M0 • Stage II – any T, N1-3, M0 • Stage III – M1
Primary Therapy – Surgery • Inguinal orchiectomy to allow high division of the spermatic cord • Scrotal approach not recommended – can alter lymphatic drainage • May not be essential for patients with bilateral tumors • Orchiectomy alone offers a cure in ~85% of patients with stage I disease
Seminoma • 70-80% of patients will present with clinical stage I disease • 15-20% have infradiaphragmatic node involvement radiologically (Stage II) • Less than 5% have distant disease
Historically… • Stage I Seminoma was treated with inguinal orchiectomy with adjuvant radiation to the paraaortic nodes • Relapse free rate of 95% • Overall survival rate of 99-100% • This rationale was to eradicate microscopic metastatic disease • However, many patients were unnecessarily radiated
Historically… • The use of surveillance for stage I NSGCT proved promising because of successful chemotherapy regimens for the relapse setting • This led to the investigation of surveillance for stage I seminoms
Surveillance • Rigshospitalet (Copenhagen) • Relapse rate of 17% at 5 years • Princess Margaret (Toronto) • Relapse rate of 15% at 5 years • Swedish Norwegian Testicular Cancer Study Group • Relapse rate of 14% with median relapse at 1.4 years • Salvage with Chemo (89%) or XRT (11%) with 1 failure • Chemo – 4 cycles cisplatin & etoposide • Primary site of relapse is in the paraaortic lymph nodes • Median time to relapse is 12-18 months though relapses after 6 years have been reported
Stage I Seminoma – Surveillance Predicting Recurrence • Warde et al, JCO 20:4448-4452, 2002 (pooled data from 4 major centers) • 5 year OS – 97.7% • 5 year CSS – 99.3% • 5 / 10 year RFS – 82.3% / 78.7%
Stage I Seminoma – Surveillance Predicting Recurrence • What factors predict recurrence? • Multivariate analysis found size >4cm (HR 2.0) and rete testis invasion (HR 1.7) predictive of relapse • 0 risk factors – 12.2% relapse • 1 risk factor – 15.9% relapse • 2 risk factors – 31.5% relapse Rete Testis 86% vs 77% SIZE 4cm 87% vs. 76%
Surveillance Schedules • ESMO (European Society for Medical Oncology) • 7 CT Scans of the abdomen over 5 years • NCCN (National Comprehensive Cancer Network) • 18 CT Scans of the abdomen/pelvis over 10 years • MRC randomized trial for surveillance (CT or MRI) • 3 in 3 years • 7 in 5 years
Stage I Seminoma - Surveillance • Surveillance – A reasonable option for stage 1 seminoma in patients who are committed to follow-up. (Warde et al JCO 13:2255, 1995, Von Der Maase et al, Eur Journ Cancer 1993;29A) • Follow up CT scans every 2-6 months for 2-3 years then less frequently • Pooled 5 year relapse rates of 18% • 84% of relapses occurred in the para-aortic nodes
Stage I Seminoma - Radiotherapy • In the modern era of post-orchiectomy radiation of the paraaortic lymph nodes… • OS rates are 92-99% • Cause-specific survival is nearly 100% • Relapse rates are 0.5-5% in modern studies (mostly supradiaphragmatic) • Most relapses occur <2 years from treatment (median 18 mo. in PMH study) • Chemotherapy is readily used in the setting of relapse
Stage I Seminoma – Radiotherapy Techniques • AP/PA field to the paraaortic and retroperitoneal lymph nodes +/- ipsalateral pelvic nodes • T10/11 superiorly to inguinal ligament inferiorly • Left renal hilum should be included for left sided tumors • Use CT to define volumes and avoid renal parenchyma • Scrotal irradiation is not required even in patients with scrotal violation
Stage I Seminoma – What Volume is Necessary • Due to low rate of pelvic node failure… • Phase II studies investigated paraaortic/RP nodal irradiation without pelvic irradiation • Showed very low rates of pelvic failure • Advantage of omitting pelvic radiation… • Decreased integral dose to patient • Decreased dose to the intact testicle!
Stage I Seminoma – Radiotherapy Volume • MRC Testicular Study Group (UK) • Fossa et al, JCO 17:1146-1154. 1999
Radiotherapy: 30 Gy/15 fx • upper border: disc - T10/T11 • lower border: mid-obturator foramen • ipsilateral margin: renal hilum to L5-S1, lateral edge of acetabulum • contralateral margin: transverse process to L5-S1, parallel to ipsilateral border, median border of obturator foramen • PA Field Identical above L5-S1
Stage I Seminoma – Radiotherapy Volume • Results • F/U 4.5 years • RFS was 96% in both arms • 4 pelvic failures – all in PA arm • 1 death from seminoma
Stage I Seminoma – Radiotherapy Volume • Paraaortic field resulted in improved • Diarrhea 7% vs 14% (p=0.013) • Leukopenia (p<0.00001) • Grade I – 14% vs 29% • Grade II – 5% vs 12% • Grade III Nausea/Emesis(p=0.08) • Time to normal sperm count improved with PA field despite more testicular shielding in DL group
Stage I Seminoma – Radiotherapy Dose • Jones et al, JCO, 23:1200-1208, 2005 • MRC/EORTC randomized 625 patients with para-aortic RT (DL if prior pelvic/scrotal surgery) to: • 30 Gy in 15 Fx, or • 20 Gy in 10 Fx • 30 Gy • 10 relapses (3 in field) • 20 Gy • 11 relapses (1 in field)
Stage I Seminoma – Radiotherapy Dose • Acute toxicity was worse with 30 Gy • Fatigue • Leukopenia • Nausea (p=0.06)
Stage I Seminoma – Chemotherapy • Oliver et al investigated the use of Carboplatin without radiation • 78 patients • 53 with 2 courses of Carbo • 25 with 1 course of Carbo • 44 months of follow up with only 1 relapse
The MRC (Oliver et at JCO, 29:957-962, 2011) randomized: With a median of 6.5 years follow up Relapse rate was 5.3% with carboplatin vs 4.0% with RT Stage I Seminoma – Chemotherapy 885 patients got PA or DL RT to between 20 and 30 Gy 560 patients got one injection of carboplatin
Stage I Seminoma – Chemotherapy • Improved fatigue with Carboplatin vs XRT • Fewer second primary GCT with Carboplatin (0.54%) vs XRT (1.96%) (p=0.04) • Paraaortic failures were the most common site with Carboplatin so surveillance imaging is required
Stage I Seminoma – Chemotherapy • Oliver et al (ASCO 2005 Abstract) • Pooled analysis of Phase II studies to compare 1 cycle vs. 2 cycles Carboplatin • Relapse Rate • 1 cycle – 4.4% • 2 cycles – 2.9% • No deaths due to seminoma
Stage I Seminoma - Outcomes • Combining the 3 randomized trials (2,466 patients) • 5 seminoma deaths for CSS of 99.8% • 4 relapses after 3 years • A prospective study of 1,192 patients treated in Sweden & Norway from 2000-2006 • 1 seminoma death for CSS of 99.9%
Stage I SeminomaSummary • Treatment • Inguinal Orchiectomy • Active Surveillance with serial imaging • ~85% RFS • 70% relapses <2years, nearly all <5 years • XRT • 95% RFS • Paraaortic equivalent with less toxicity than PA/Pelvic (dog leg) • 20 Gy equivalent with less toxicity than 30 Gy • Carboplatin • 95% RFS • One cycle equivalent to two cycles
Stage II Seminoma • Stage IIA – RP node <2cm • Stage IIB – RP node 2.1-5cm • Stage IIC - >5 cm • Few patients have stage II disease making randomized trials difficult to perform • Data hence stems from institutional experiences • The greatest prognostic factor is bulk of nodal disease (diameter of largest node)
Stage II Seminoma • NCCN guidelines recommend EBRT to RT to the para-aortics and ipsilateraliliacs (dogleg) to 35-40 Gy • PMH has reported on 95 pts treated in this way between 1981-1999 • 91% RFS with <5cm node • 44% RFS with >5cm node • Relapse most common in mediastinum, SCF, lung, bone • 70% salvaged with chemotherapy
Residual Retroperitoneal Mass • Presence of residual masses after definitive treatment is common • Most often represent fibrosis or necrosis • Very few contain viable tumor • Options • Observation • Surgery • RT (after chemo) • PET is of little value in this setting
Residual Retroperitoneal Mass • MSKCC studies patients with residual RP masses and the role of surgery or biopsy • 0% of patients with mass <3cm had viable tumor • These patients should be observed • 30% of patients with mass >3cm had viable tumor • Biopsy residual mass or… • Observe with serial CT • Treat with enlarging mass
Residual Retroperitoneal Mass • Horwich et al reported 29 patients with residual RP mass following platinum-based chemotherapy • 15 treated with adjuvant XRT • 14 observed • No evidence that adjuvant XRT decreased relapse rate • MRC pooled 123 patients residual mass • 56% treated with adjuvant XRT • 44% observed • No evidence that adjuvant XRT decreased relapse rate
Stage II Seminoma • XRT yields RFS of 90% with PA/Pelvis fields • Platinum based chemotherapy can be used with adjuvant XRT showing no benefit • Residual RP mass • <3cm - nearly always fibrotic – observe • >3cm – 30% residual tumor – biopsy or serial CT
Stage IIC - III Seminoma • These patients are uncommon (5%) • 40-50% relapse rate for IIC patients treated with EBRT alone • 4 cycles of Cisplatin/Etoposide has yielded 92% freedom from progression at MSKCC and is considered the standard approach
Targeted Therapy • Scientists evaluating cell surface molecules and mutations associated with GCT • No targeted therapy in clinical use • With high RFS, CSS, OS rates, targeted therapy is not likely to be beneficial or cost effective
Proton Therapy • Dosimetric models suggest that there is decreased normal tissue exposure with protons • No patients being treated with protons • Not cost effective
Fertility • 50 percent of men with testicular cancer have some impairment of spermatogenesis (more with NSGCT than seminoma) • All patients should have sperm analysis with option of cryopreservation prior to adjuvant therapy • RT patients should have shielding of the contralateral testicle
Fertility & Radiation • Temporary azospermia can occur with 2 Gy • Permanent azospermia after ~7 Gy • Stem cells are the most sensitive to XRT resulting in azospermia • Leydig cells (testosterone producing cells) have a much higher tolerance so patients rarely suffer from hypotestosterone from XRT
Fertility • Norwegian study of 1,814 patients • 554 attempted natural conception • Equal rates of conception with RT compared to retroperitoneal LN dissection (~80%)