Download
1 / 1
10 likes | 302 Views
TUMOR CHARACTERISTICS. INTRODUCTION TO ENDOSCOPIC SKULL BASE SURGERY. Mohamed S. Kabil, MD Hrayr K. Shahinian, MD, FACS. Introduction

E N D
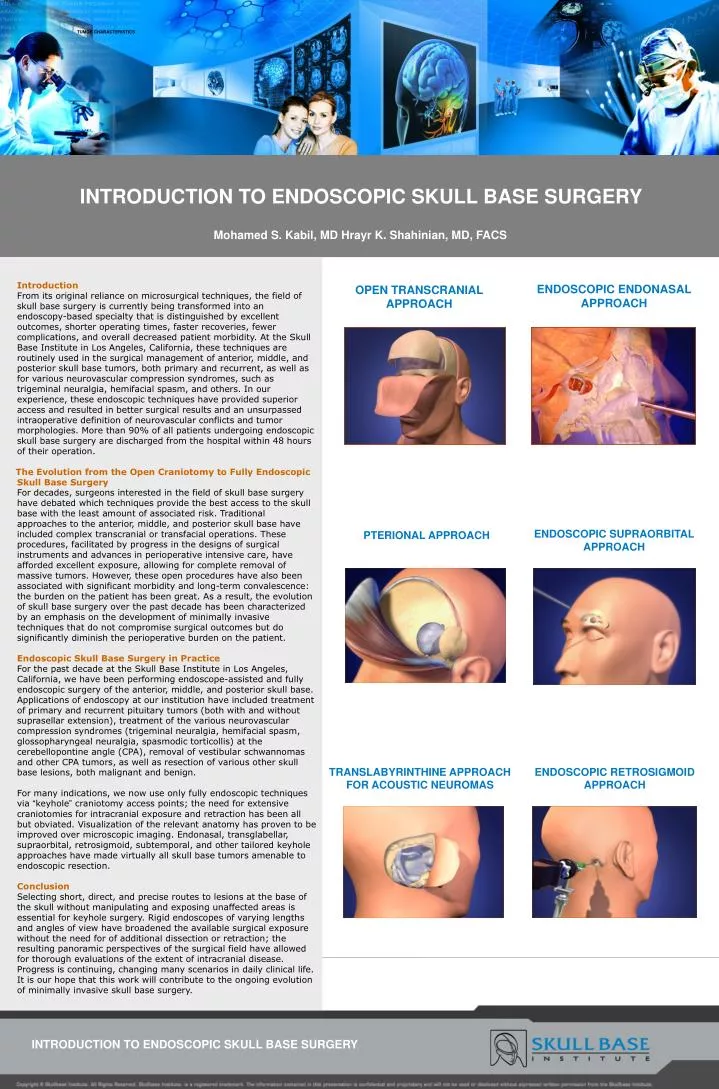
TUMOR CHARACTERISTICS INTRODUCTION TO ENDOSCOPIC SKULL BASE SURGERY Mohamed S. Kabil, MD Hrayr K. Shahinian, MD, FACS Introduction From its original reliance on microsurgical techniques, the field of skull base surgery is currently being transformed into an endoscopy-based specialty that is distinguished by excellent outcomes, shorter operating times, faster recoveries, fewer complications, and overall decreased patient morbidity. At the Skull Base Institute in Los Angeles, California, these techniques are routinely used in the surgical management of anterior, middle, and posterior skull base tumors, both primary and recurrent, as well as for various neurovascular compression syndromes, such as trigeminal neuralgia, hemifacial spasm, and others. In our experience, these endoscopic techniques have provided superior access and resulted in better surgical results and an unsurpassed intraoperative definition of neurovascular conflicts and tumor morphologies. More than 90% of all patients undergoing endoscopic skull base surgery are discharged from the hospital within 48 hours of their operation. The Evolution from the Open Craniotomy to Fully Endoscopic Skull Base Surgery For decades, surgeons interested in the field of skull base surgery have debated which techniques provide the best access to the skull base with the least amount of associated risk. Traditional approaches to the anterior, middle, and posterior skull base have included complex transcranial or transfacial operations. These procedures, facilitated by progress in the designs of surgical instruments and advances in perioperative intensive care, have afforded excellent exposure, allowing for complete removal of massive tumors. However, these open procedures have also been associated with significant morbidity and long-term convalescence: the burden on the patient has been great. As a result, the evolution of skull base surgery over the past decade has been characterized by an emphasis on the development of minimally invasive techniques that do not compromise surgical outcomes but do significantly diminish the perioperative burden on the patient. Endoscopic Skull Base Surgery in Practice For the past decade at the Skull Base Institute in Los Angeles, California, we have been performing endoscope-assisted and fully endoscopic surgery of the anterior, middle, and posterior skull base. Applications of endoscopy at our institution have included treatment of primary and recurrent pituitary tumors (both with and without suprasellar extension), treatment of the various neurovascular compression syndromes (trigeminal neuralgia, hemifacial spasm, glossopharyngeal neuralgia, spasmodic torticollis) at the cerebellopontine angle (CPA), removal of vestibular schwannomas and other CPA tumors, as well as resection of various other skull base lesions, both malignant and benign. For many indications, we now use only fully endoscopic techniques via “keyhole” craniotomy access points; the need for extensive craniotomies for intracranial exposure and retraction has been all but obviated. Visualization of the relevant anatomy has proven to be improved over microscopic imaging. Endonasal, transglabellar, supraorbital, retrosigmoid, subtemporal, and other tailored keyhole approaches have made virtually all skull base tumors amenable to endoscopic resection. ConclusionSelecting short, direct, and precise routes to lesions at the base of the skull without manipulating and exposing unaffected areas is essential for keyhole surgery. Rigid endoscopes of varying lengths and angles of view have broadened the available surgical exposure without the need for of additional dissection or retraction; the resulting panoramic perspectives of the surgical field have allowed for thorough evaluations of the extent of intracranial disease. Progress is continuing, changing many scenarios in daily clinical life. It is our hope that this work will contribute to the ongoing evolution of minimally invasive skull base surgery. ENDOSCOPIC ENDONASAL APPROACH OPEN TRANSCRANIAL APPROACH ENDOSCOPIC SUPRAORBITAL APPROACH PTERIONAL APPROACH TRANSLABYRINTHINE APPROACH FOR ACOUSTIC NEUROMAS ENDOSCOPIC RETROSIGMOID APPROACH INTRODUCTION TO ENDOSCOPIC SKULL BASE SURGERY