Download

1 / 45
490 likes | 829 Views
Ovarian & Menstrual Cycles. Objectives:. understand the hypothalmo-pituitary-ovarian axis Understand the ovarian/menstrual cycles with the hormonal interaction in the normal subject.

E N D
Ovarian & Menstrual Cycles
Objectives: • understand the hypothalmo-pituitary-ovarian axis • Understand the ovarian/menstrual cycles with the hormonal interaction in the normal subject. • Understand the clinical significance and implication in different aspect of gynecological abnormalities and treatments
Menstruation is Greek word that means toxin. It is periodic uterine blood loss during reproductive years of women. It is the red badge of femininity. Definition
Two types; ovular or true menstruation and anovular or false menstruation. Two phases; proliferative phase and secretory phase. The mean duration of the flow is 5 3 days and the average menstrual blood loss is 50 ml (20-80 mls). The cycle is 28 7 days. The mean age of menarche is 12.7 years Features of menstruation
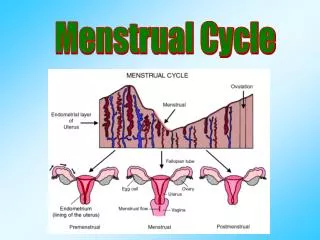
This phase lasts from the first day of menses until ovulation During this phase the endometrium (zona functionalis) proliferates under the effect of E2 & IGF-1 Characteristics Variable length Low BBT Developing ovarian follicles Estrogen production (G-cells) Vascular growth of the endometrium Proliferative phase
This phase Extend from ovulation until the onset of the next menses. During this phase the endometrium show secretory changes under the effect of 4p. Characteristics Constant length 14 days High BBT Formation of corpus luteum The endometrium show tortuous secretory glands full of glycogen in preparation for nidation. Secretory phase
Endometrial histology Proliferative phase Secretory phase
The endometrium is divided into two zones the basal one does not share in menstruation but it the regenerative layer and the functional zone that is shed during menstruation. Progesterone withdrawal brings neutrophil accumulation that dissociate the endometrial stroma and the release of PGF2- that cause vasospasm of the contraction cone of Markee The necrosed segment of the endometrium is washed out during menstruation. Menstruation
For proper menses to occur there should be a nice integration between the hypothalamus, pituitary, ovary and responsive uterus as well as a patent effluent genital tract. Hormones integrated GnRH FSH/LH E2/ 4p Endocrine control of menstruation
Hypothalamus Hypothalamus Pituitary Stalk Pituitary gland
Hypothalamic control of gonadotropin secretion is exerted via the release of gonadotropin-releasing hormone .GnRH is a small peptide consisting of 10 amino acids (decapeptide). GnRH neurons migrate into the brain from the embryonic olfactory placodes, where they are first observed, to reach the locations they will occupy during adult life (hypothalamus). GnRH is known to release both LH and FSH both LH and FSH are released in a pulsatile rather than a continuous fashion. Each pulse of LH consists of the abrupt release of the hormone from the gonadotrope into the peripheral circulation, followed by an exponential decline representative of the hormone's half-life. Pulsatile gonadotropin release is not the result of an intrinsic property of the anterior pituitary gland but is causally related to the pulsatile release of GnRH (the GnRH pulse generator). GnRH
Only intermittent GnRH administration produces sustained increases in both gonadotropins; continuous exposure, even to high doses of GnRH, rapidly produces a desensitization of the gonadotrope, resulting in a lowering of LH and FSH release and the arrest of reproduction function A high GnRH pulse frequency favors LH synthesis and release, but a low GnRH frequency favors FSH synthesis and secretion GnRH
GnRH gene is 5 kb on Ch 8p Signal peptide GnRH GAP GnRH gene product Precursor peptide (Pre-pro-GnRH) 23 aa 10 aa 3 aa 56 aa Proteolytic Stimulates FSH/LH Inhibits PRL NB: Mutation in prohormone convertase 1 (PC1) gene results in insulin resistance
Arcuate venteromedial nucleus Neural control of GnRH High Amplitude High Frequency GnRH Follicular phase Luteal phase NB: A critical GnRH pulse frequency and amplitude is needed for proper menstruation
FSH-R are found primarily on granulosa cells FSH stimulates follicular growth (gametokinetic) FSH stimulates aromatase enzyme system in the granulosa cells and hence estrogen production Granulosa cells acquire LH receptors just before ovulation. FSH receptors
LH-R are found on theca cells at all stages of the cycle and on granulosa cells just before ovulation LH stimulates androgen production by theca cells When sufficient number of LH-R are acquired on granulosa cells, LH stimulates luteinization and progesterone production. LH receptors
Feedback Regulation of Gonadotropin secretion the major feedback loop is inhibitory (negative feedback loop): steroid hormones (estradiol and progesterone) secreted by the target organ (the ovary) “feed back” to the hypothalamic-hypophyseal unit to adjust GnRH and gonadotropin secretion Estradiol 17β is a potent physiologic inhibitor of GnRH and of gonadotropin secretion. levels of LH and FSH during the follicular phase are characteristically determined by the changes in estradiol concentrations that accompany maturation of the follicle. As circulating estradiol levels increase, gonadotropin concentrations decrease
The estradiol negative feedback loop acts to decrease LH secretion mainly by controlling the amplitude of the LH pulse. Thus, as the follicular phase progresses, LH pulse amplitude declines. LH pulse frequency during the follicular phase (at intervals of 60 to 100 minutes), suggesting that estradiol does not particularly affect LH pulse frequency Feedback Regulation of Gonadotropin secretion
During the estrogenic stage or follicular phase, pulses of high frequency but of low amplitude are seen; during the progesterone stage or luteal phase, there is a great reduction in the frequency of the LH pulse, with pulse intervals of 200 minutes or more. This decreased pulse frequency is accompanied by a significant increase in pulse amplitude. Feedback Regulation of Gonadotropin secretion
Patterns of pulsatile luteinizing hormone (LH) secretion during the human menstrual cycle. (A) Note the high frequency of pulsatile LH release. (B) Note the reduction in pulse frequency, with a corresponding increase in pulse amplitude.
Two cell hypothesis (Short 1963) • Two hormones • LH • FSH • Two cells • Theca cell • Granulosa cell • Two products • E1 • E2 Theca cell Cholesterol LH cAMP AD Te Granulosa cell AD Te FSH cAMP Aromatization E1 E2
THE FOLLICULAR PHASE Recruitment of a Follicle Cohort Selection of the Dominant Follicle Growth of the Dominant Follicle OVULATION THE LUTEAL PHASE Oogenesis
Oogenesis • Primordial follicle • Growing follicle • Preantral follicle • Antral follicle • Mature Graafian follicle • Ovulation • Corpus luteum
Primordial follicle An oocyte arrested in in the diplotene stage of first meiotic prophase surrounded by a single layer of granulosa cells Initial follicular growth is independent of hormone The oocyte stock at the beginning of reproductive life is 360,000. Oogenesis
Preantral follicle An oocyte surrounded by the ZP and several layers of granulosa cells and theca cells FSH rescue some preantral follicles from atresia and stimulate their growth, this may span more than one cycle FSH induces aromatization of thecal androgen in the granulosa cells Estrogen stimulates more follicular growth and induces more FSH-R on granulosa cells. Oogenesis
Antral follicle Fluid accumulates in between granulosa cell (Call-Exner) that coalese to form the antrum Follicle destined to become dominant secretes more estrogen that induces more FSH-R. Dominant follicle continues to grow in spite of declining level of FSH due to high receptor content Other follicles fail to do so and testosterone accumulates to bring their atresia. Oogenesis
Established and Putative Intraovarian Regulators Insulin-Like Growth Factor System IGF-I IGF-II IGF binding proteinsInhibin/Activin Systems Inhibin Activin FollistatinInterleukin-1 System Interleukin-1 Interleukin-1 receptor antagonist IL-1 binding protein (IL-1 receptor type II) Other Growth Factors EGF/TGFα TGFβ1, TGFβ2 NGF aFGF, bFGF VEGF TNFαOther Peptidergic Factors Ovarian renin angiotensin system VIP Oxytocin Endothelin
Principal Actions of Intraovarian Regulators Insulin-like growth factor-I Follicle-stimulating hormone (FSH) amplification Follicular growth Follicular selection Transforming growth factor-α Follicular maturation Oocyte maturation Cellular differentiation Potentiation of gonadotropin action Regulation of apoptosis
Principal Actions of Intraovarian Regulators Transforming growth factor-β1 Follicular rupture inhibition Follicular differentiation Basic fibroblast growth factor Apoptosis inhibition Regulation of folliculogenesis Activin Oocyte maturation Follicular differentiation Early embryogenesis Regulation of steroidogenesis
Principal Actions of Intraovarian Regulators Interleukin-1 Ovulation induction Glycolysis Glucose transport Tumor necrosis factor-α Inhibits steroidogenesis FSH antagonist Induces apoptosis/luteolysis Ovulation inhibition
This is the follicle of the month destined to ovulate The capacity of this follicle to aromatize is vast. When the follicle reaches maturity 18-20 mm, the estrogen level is of magnitude -200 pg/ml for 50 hours- to trigger LH surge and ovulation follows 12 hours after the peak. Mature Graafian follicle
LH surge triggers ovulation, it is a slow process and involves enzymatic digestion of the follicular wall LH surge Resumption of meiosis Luteinization of granulosa cells Prostaglandin synthesis Mid-cycle rise of FSH is progesterone dependant and loosens the oocyte in its bed so it becomes free floating in the antral fluid It is the secondary oocyte and first polar body that come out at ovulation. Ovulation
The corpus luteum is formed after ovulation under tonic effect of LH Granulosa layer is invaded by blood vessels after breakdown of the membrana limitans. Granulosa cells increase in size accumulate lutein and secrete progesterone. Progesterone peaks at LH+7, levels > 10 ng/ml indicate proper ovulation. Ten days post ovulation the corpus luteum begins to decline unless hCG appears. Corpus luteum