Download
1 / 98
980 likes | 1.13k Views
Diseases of White Blood Cells(2). Lecturer :Yiran Ni, MD Department of Pathology China Three Gorges University Email:nyr1986@gmail.com. Dec.2012. What we’ve learned. Leukopenia; Reactive leukocytosis; Lymphadenitis;

E N D
Diseases of White Blood Cells(2) Lecturer :Yiran Ni, MD Department of Pathology China Three Gorges University Email:nyr1986@gmail.com Dec.2012
What we’ve learned • Leukopenia; • Reactive leukocytosis; • Lymphadenitis; • General aspects and classification of neoplastic proliferation of white cell; • Acute myeloid leukaemia
Target of this class • Myelodysplastic Syndromes • chronic myeloid leukaemia • histiocytoses • splenomegaly
General aspect • The term "myelodysplastic syndromes" (MDS) refers to a group of clonal stem cell disorders characterized by maturation defects associated with ineffective hematopoiesis and an increased risk of transformation to acute myelogenous leukemias (AML).
General aspect • In patients with MDS, the bone marrow is partly or wholly replaced by the clonal progeny of a mutant multipotent stem cell that retains the capacity to differentiate into red cells, granulocytes, and platelets but in an ineffective and disordered fashion. • These disturbances usually manifest as peripheral blood cytopenias.
General aspect • In patients with MDS, the bone marrow is partly or wholly replaced by the clonal progeny of a mutant multipotent stem cell that retains the capacity to differentiate into red cells, granulocytes, and platelets but in an ineffective and disordered fashion. • These disturbances usually manifest as peripheral blood cytopenias.
General aspect • MDS arises in two distinct settings: • Idiopathic or primary MDS occurs mainly at ages over 50 and often develops insidiously. • Therapy-related MDS (t-MDS) is a complication of previous genotoxic drug or radiation therapy that appears 2 to 8 years after treatment.
General aspect • All forms of MDS can transform to AML, but transformation occurs most rapidly and with highest frequency in t-MDS. • Although characteristic morphologic changes are typically seen in the marrow and the peripheral blood, definitive diagnosis frequently requires correlation with other laboratory tests. • Cytogenetic analysis is particularly helpful in confirming the diagnosis, as certain chromosomal aberrations are often observed.
Pathogenesis • The pathogenesis of MDS is unknown. • Although the marrow is usually hypercellular at diagnosis, it can also be normocellular or, less commonly, hypocellular.
Pathogenesis • Myelodysplastic bone marrow progenitors undergo apoptotic cell death at an increased rate, the hallmark of ineffective hematopoiesis. • Given this, it is difficult to understand how myelodysplastic progenitors could displace any remaining normal marrow progenitors, suggesting that MDS arises within a background of stem cell damage or depletion.
Pathogenesis • Both primary MDS and t-MDS occurring after exposure to radiation or alkylating chemotherapeutic drugs are associated with similar clonal chromosomal abnormalities, including monosomy 5 and monosomy 7, deletions of 5q and 7q, trisomy 8, and deletions of 20q.
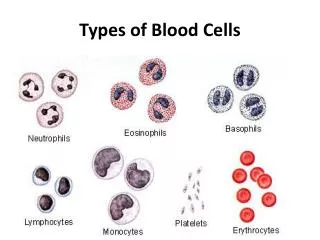
Morphology • The most characteristic finding is disordered (dysplastic) differentiation affecting all non-lymphoid lineages (erythroid, granulocytic, monocytic, and megakaryocytic)
Morphology • Within the erythroid series, common abnormalities include: ringed sideroblasts, erythroblasts with iron-laden mitochondria visible as perinuclear granules in Prussian blue-stained biopsies; megaloblastoid maturation resembling that seen in vitamin B12 and folate deficiency; and nuclear budding abnormalities, recognized as nuclei with misshapen, often polypoid, outlines
Morphology • Neutrophils often contain decreased numbers of secondary granules, toxic granulations. • neutrophils with only two nuclear lobes, are frequently observed, and neutrophils may even be seen that completely lack nuclear segmentation.
Morphology • Megakaryocytes with single nuclear lobes or multiple separate nuclei (pawn ball megakaryocytes) are also characteristic. • Myeloblasts may be increased but make up less than 20% of the overall marrow cellularity.
Morphology • The peripheral blood often contains pseudo-Pelger-Hüet cells, giant platelets, macrocytes, poikilocytes, and a relative or absolute monocytosis. • Myeloblasts usually make up less than 10% of the peripheral leukocytes.
A, Nucleated red cell progenitors with multilobated or multiple nuclei • C, Pseudo-Pelger-Hüet cells, neutrophils with only two nuclear lobes instead of the normal three to four, are observed at the top and bottom of this field. D, Megakaryocytes with multiple nuclei instead of the normal single multilobated nucleus B, Ringed sideroblasts, erythroid progenitors with iron-laden mitochondria, seen as blue perinuclear granules
Clinical Course • Primary MDS affects mainly individuals older than 60 years of age. • When symptomatic, it presents with weakness, infections, and hemorrhages, all due to pancytopenia. • In up to half of the cases, MDS is discovered incidentally on routine blood testing.
Clinical Course • The median survival in primary MDS varies from 9 to 29 months. • Overall, progression to AML occurs in 10% to 40% of individuals and is often accompanied by the appearance of additional clonal cytogenetic changes. • Patients often succumb to the complications of thrombocytopenia (bleeding) and neutropenia (infection
Clinical Course • The outlook is even grimmer in t-MDS, which has an overall median survival of only 4 to 8 months. Cytopenias tend to be more severe than in primary MDS, and progression to AML is often rapid.
Clinical Course • Treatment options in MDS are limited. • In younger patients, allogeneic bone marrow transplantation offers some hope for reconstitution of normal hematopoiesis and long-term survival. • Older patients with MDS are treated supportively with antibiotics and blood product transfusions
Chronic Myeloproliferative Disorders/ Chronic Myelogenous Leukemia
General aspects of CMD • In most disorders of this group, the neoplastic cell is a multipotent progenitor cell that is capable of giving rise to mature erythrocytes, platelets, granulocytes, monocytes. • The only exception is chronic myelogenous leukemia, in which the pluripotent stem cell that gives rise to lymphoid and myeloid cells is affected.
General aspects of CMD • As in AML, the neoplastic cells and their offspring flood the bone marrow and suppress residual normal progenitor cells; • however, in the chronic myeloproliferative disorders, terminal differentiation is relatively unaffected. This combination leads to marrow hypercellularity and increased hematopoiesis, often accompanied by elevated peripheral blood counts.
Classification • The four most common chronic myeloproliferative disorders (MPDs) are: • (1) chronic myelogenous leukemia • (2) polycythemia vera • (3) essential thrombocytosis • (4) primary myelofibrosis.
Classification • All four have some similar features.: • The neoplastic stem cells have the capacity to circulate and home to secondary hematopoietic organs, particularly the spleen, where they give rise to extramedullary hematopoiesis. As a result, all chronic MPDs cause varying degrees of splenomegaly.
Classification • They also share the propensity to terminate in a spent phase characterized by marrow fibrosis and peripheral blood cytopenias. • Further, all can progress over time to acute leukemia, but only chronic myelogenous leukemia (CML) does so invariably.
General aspects of CML • Chronic myelogenous leukemia (CML) is a disease primarily of adults between the ages of 25 and 60 years, with the peak incidence in the fourth and fifth decades of life.
Pathophysiology • CML is distinguished from other chronic MPDs by the presence of a distinctive molecular abnormality; • namely, a translocation involving the BCR gene on chromosome 9 and the ABL gene on chromosome 22. The resultant BCR-ABL fusion gene directs the synthesis of a 210-kDa fusion protein with tyrosine kinase activity. • .
Pathophysiology • In more than 90% of CML cases, karyotyping reveals the so-called Philadelphia chromosome (Ph), which is created by a reciprocal (9;22)(q34;q11) translocation. • However, in 5% to 10% of cases, the rearrangement is complex or cytogenetically cryptic; in such cases, other methods such as FISH RT-PCR can be used to detect the BCR-ABL fusion gene or transcript.
Ph BCR-ABL fusion gene tyrosine kinase cell division and inhibition of apoptosis
Pathophysiology • Introduction of the BCR-ABL fusion gene into murine bone marrow cells gives rise to a syndrome resembling human CML; hence, its acquisition is considered to be a critical pathogenetic event.
Pathophysiology • The activity of diverse tyrosine kinases is normally regulated by ligand-mediated dimerization, followed by the activation of multiple downstream pathways, which control cell survival and proliferation. • Detailed molecular dissection has shown that BCR contributes a dimerization domain that promotes self-association of the BCR-ABL fusion protein, resulting in constitutive BCR-ABL autophosphorylation and activation of downstream pathways.
Pathophysiology • The net effect of these events is cell division and inhibition of apoptosis, independent of ligand binding. Such autonomous triggering contributes to unregulated myeloproliferation
Pathophysiology • In CML, multiple myeloid lineages, B lymphoid cells and possibly T lymphoid cells express the BCR-ABL fusion protein, indicating that the target of transformation is a pluripotent stem cell. • For unknown reasons, the effect of the constitutively active BCR-ABL kinase early in the course of CML is evident mainly in granulocytic progenitors and, to a lesser degree, in megakaryocytic progenitors.
Morphology • In contrast to normal bone marrow, which is usually about 50% cellular and 50% fat, CML marrows are usually 100% cellular, with maturing granulocytic precursors comprising most of the increased cellularity. • Increased numbers of megakaryocytes, often including small dysplastic forms, are also frequently observed, whereas erythroid progenitors are usually present in normal or decreased numbers.
Morphology • A characteristic finding is the presence of scattered storage histiocytes with wrinkled, green-blue cytoplasm (sea-blue histiocytes). • Increased deposition of reticulin fibers is typical, but overt marrow fibrosis is rare at presentation.
Morphology • Peripheral blood examination reveals a marked leukocytosis, often exceeding 100,000 cells per mm3. The circulating cells are predominantly neutrophils, metamyelocytes, and myelocytes, with less than 10% myeloblasts. • Peripheral blood eosinophilia and basophilia are also common, and up to 50% of patients have thrombocytosis early in the course of their disease.
Morphology • Neoplastic extramedullary hematopoiesis within the splenic red pulp produces marked splenomegaly , often complicated by focal infarction. Extramedullary hematopoiesis can also lead to hepatomegaly and mild lymphadenopathy.
Clinical Features • The onset of CML is insidious. • Mild-to-moderate anemia and hypermetabolism due to increased cell turnover lead to easy fatigability, weakness, weight loss, and anorexia. • Sometimes the first symptom is a dragging sensation in the abdomen caused by the extreme splenomegaly, or acute onset of left upper quadrant pain due to splenic infarction.
Clinical Features • CML is best differentiated from other chronic myeloproliferative disorders by detection of the BCR-ABL fusion gene, through either chromosomal analysis or PCR-based molecular tests.
Clinical Features • The natural history of CML is one of slow progression, and even without treatment, a median survival of 3 years can be expected. • After a variable period averaging 3 years, approximately 50% of patients enter an "accelerated phase," during which there is increasing anemia and thrombocytopenia and sometimes striking peripheral blood basophilia.
Clinical Features • Additional clonal cytogenetic abnormalities, such as trisomy 8, isochromosome 17q, or duplication of the Ph, can also appear. • Within 6 to 12 months, the accelerated phase terminates in a picture resembling acute leukemia (blast crisis). • In the remaining 50%, blast crises occur abruptly without an intermediate accelerated phase.
Clinical Features • In 70% of blast crises, the blasts have the morphologic and cytochemical features of myeloblasts, whereas in most of the remainder, the blasts contain the enzyme TdT and express early B-lineage markers such as CD10 and CD19. Rarely, the blasts resemble precursor T cells. • These observations further support the notion that the target cell for transformation is a pluripotent stem cell.
Clinical Features • Understanding of the molecular pathogenesis of CML has led to the introduction of drugs that inhibit the BCR-ABL kinase, which induce complete hematologic remissions in more than 90% of patients. • However, BCR-ABL inhibitors suppress but do not extinguish the CML clone and, as a result, may not prevent progression to blast crisis.
Clinical Features • Moreover, while patients in blast crisis initially respond to BCR-ABL kinase inhibitors, they recur rapidly with refractory disease. • For these reasons, allogeneic bone marrow transplantation, which is most effective when performed in the stable phase, is the favored treatment in younger patients. Of those with a suitable donor, about 75% are cured.