Download
1 / 2
20 likes | 331 Views
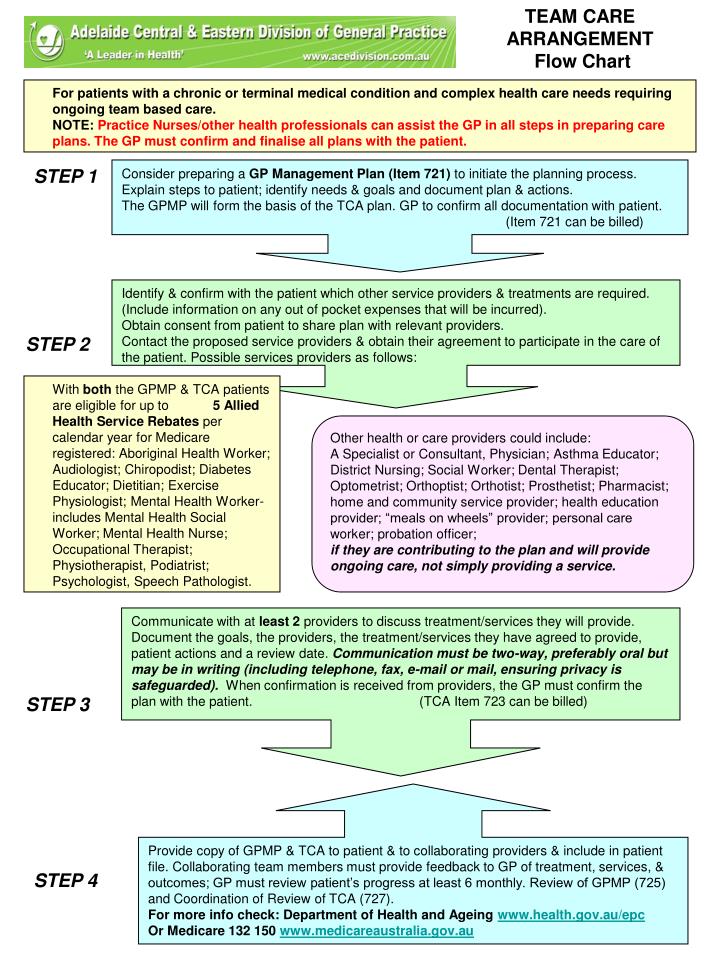
TEAM CARE ARRANGEMENT Flow Chart. For patients with a chronic or terminal medical condition and complex health care needs requiring ongoing team based care.

E N D
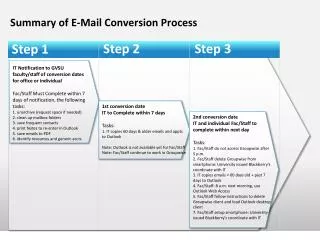
TEAM CARE ARRANGEMENT Flow Chart • For patients with a chronic or terminal medical condition and complex health care needs requiring ongoing team based care. • NOTE: Practice Nurses/other health professionals can assist the GP in all steps in preparing care plans. The GP must confirm and finalise all plans with the patient. Consider preparing a GP Management Plan (Item 721) to initiate the planning process. Explain steps to patient; identify needs & goals and document plan & actions. The GPMP will form the basis of the TCA plan. GP to confirm all documentation with patient. (Item 721 can be billed) STEP 1 Identify & confirm with the patient which other service providers & treatments are required. (Include information on any out of pocket expenses that will be incurred). Obtain consent from patient to share plan with relevant providers. Contact the proposed service providers & obtain their agreement to participate in the care of the patient. Possible services providers as follows: STEP 2 • With both the GPMP & TCA patients are eligible for up to 5 Allied Health ServiceRebates per calendar year for Medicare registered: Aboriginal Health Worker; Audiologist; Chiropodist; Diabetes Educator; Dietitian; Exercise Physiologist; Mental Health Worker-includes Mental Health Social Worker; Mental Health Nurse; Occupational Therapist; Physiotherapist, Podiatrist; Psychologist, Speech Pathologist. Other health or care providers could include: A Specialist or Consultant, Physician; Asthma Educator; District Nursing; Social Worker; Dental Therapist; Optometrist; Orthoptist; Orthotist; Prosthetist; Pharmacist; home and community service provider; health education provider; “meals on wheels” provider; personal care worker; probation officer; if they are contributing to the plan and will provide ongoing care, not simply providing a service. Communicate with at least 2 providers to discuss treatment/services they will provide. Document the goals, the providers, the treatment/services they have agreed to provide, patient actions and a review date. Communication must be two-way, preferably oral but may be in writing (including telephone, fax, e-mail or mail, ensuring privacy is safeguarded).When confirmation is received from providers, the GP must confirm the plan with the patient. (TCA Item 723 can be billed) STEP 3 Provide copy of GPMP & TCA to patient & to collaborating providers & include in patient file. Collaborating team members must provide feedback to GP of treatment, services, & outcomes; GP must review patient’s progress at least 6 monthly. Review of GPMP (725) and Coordination of Review of TCA (727). For more info check: Department of Health and Ageing www.health.gov.au/epc Or Medicare 132 150 www.medicareaustralia.gov.au STEP 4
GP refers eligible patient to CDE* or AEP* or APD* or Practice known be involved in group services under the Medicare Group Item, to be assessed for suitability for a preferred group intervention. CDE or AEP or APD individually assesses the patient for suitability and prepares for group services. Patients unsuitable for groups may be screened out at this time. Report: to GP on assessment undertaken, suitability for group services, nature of proposed group services Allied Health group services under Medicare for patients with type 2 diabetes STEP 1: Referral STEP 2: Individual Assessment CDE and/or AEP and/or APD conduct group sessions. A maximum 8 sessions per calendar year. Sessions must include 2-12 Medicare patients. Non-Medicare, full-paying patients can also attend. Report: after last service to referring GP for each Medicare patient. STEP 3: Group Services Taken from AGPN website: www.adgp.com.au PowerPoint Presentation April 2007 *CDE-Credentialled Diabetes Educator *AEP- Accredited Exercise Physiologist *APD- Accredited Practicing Dietitian Insert Logos of all 3 Practitioner types in order of CDE, AEP & APD