Download
1 / 21
240 likes | 604 Views
Hemolytic Anemia by Areej T.Kadhum. Haemolysis. Normal life span of a RBC is 120 days (80-90 days in a full term infant). Senescent RBC is detected & cleared by RE. Reduced/shortened life span = premature cell destruction + No marrow compensation Abnormal hemolysis

E N D
Haemolysis • Normal life span of a RBC is 120 days (80-90 days in a full term infant). Senescent RBC is detected & cleared by RE. • Reduced/shortened life span = premature cell destruction + No marrow compensation Abnormal hemolysis Hemolytic Anemia is a condition in which the blood has a low number of erythrocytes due to premature destruction of RBCs coupled with increased erythropoieses.
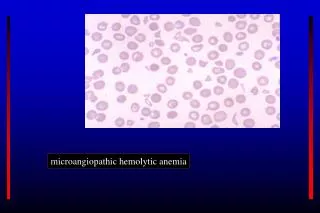
Classification • There are many types of hemolytic Anemia, classified according to the site of RBC destruction-Intravascular or Extravascular & cause of hemolysis. • the causing factors can be Intrinsic (defect is within the cell) or Extrinsic ( external impact) • Intrinsic factor is Inherited . Extrinsic is often acquired.
Inherited (ntracorpuscular) Acquired (extracorpuscular) Immune mediated: Alloimmune : Rh incompatibility and ABO hemolytic disorders Oxidant drugs induced hemolysis (primaquine) Autoimmune: Infections such as hep. C ,HIV , Malaria,tuberculosis. Burns Microangiopathy Transfusion reaction. • Enzymopathies (Deficiency of G6PD , pyruvate kinase,hexokinase def.) • Defects of red cell membrane: spherocytosis,elliptocytosis acanthocytosis • Hemoglobinopathies,sickle cell,hemoglobin E disease. • Infantile pyknocytosis
Cytoskeleton of RBC • Note the Spectrin mesh like pattern , main demonstrating protein on the membrane. Together with ankyrin maintain the normal bi concave shape of the cell, if any defect of spectrin - reduced density of membrane skeleton, (spheroid RBC ) recognized by RE as abnormal shaped and destoyed in the spleen
Favism linked to hemolytic G6PD deficiency Opss! Avoid fava beans in type II G6PD def. Most common in Mediterranean countries, south Europe and Middle East
Diagnosis of HA Symptoms depend on degree & severity of hemolysis (the rate of destruction) Clinical features: general anemia symptoms (fatigue,dyspnea,palpitations, postural dizziness, cold extremities etc), In severe phases: lemon yellowish sclera & jaundice Lab. Findings: reticulocytosis , high MCV, elevated indirect bilirubin, elevated LDH, low haptoglobin, positive DAT (Coomb’s test) in AIHA, negative in non-immune mediated types. Acute intravascular hemolysis: fever, chills, low back pain, hemoglobinuria, & hemosiderinuria( usually seen 3-4 days after the onset of hemolytic conditions) Blood Smear: polychromatophilia (a sign of b.marrow stress), spherocytosis & autoagglutination
Intravascular hemolysis event: • Immediate drop in Haptoglobin; rises at 2 days • Hemoglobinemia detectable 6-12 hrs post hemolytic phase • Hemoglobinuria detectable 12-24 hrs • Hemosiderinuria detectable 3-12 days • Methemalbumin detectable 1-12 days
Drug-induced Hemolysis • May occur by an immune mechanism or by challenging the RBC metabolic machinery • Oxidant drugs causing hemolysis in G6PD deficiency: sulfa drugs,anti-pyretics, dapsone, primaquine, pyridium, doxorubicin • Drugs causing immune-mediated hemolysis: penicillin, quinidine, methyldopa, streptomycin
Drug Induced Hemolysis • Formation of antibodies specific to the drugs: in high dosesof PCN bind proteins on RBC membrane, patient forms Ab against PCN- RBC is destroyed. • Induction of Abs to RBC membrane antigens:methyldopa induces autoAb to Rh Ag • Selective binding of streptomycin to RBC membrane with formation of complement fixing antibody • All have Coombs (DAT) positive for IgG
Immune Complex Mechanism • Drug and antibody bind in the plasma • This Immune complex will either • Activate complement in the plasma, or • Choose a RBC surface to occupy • Antigen-antibody complex recognized by RE system • RBC is destroyed as “innocent bystander” of destruction of immune complex.
Compatibility check before graft & transfusion • ABO & Rh Type of both donor & recipient • Antibody Screen of Donor & Recipient, including indirect Coombs • Major cross-match by same procedure (recipient serum & donor red cells),performed if no clear result from the easier screening tests.
AlloimmuneHemolysisHemolytic Disease of the Newborn • Due to incompatibility between mother negative for an antigen & fetus + his father r positive for that antigen. Rh incompatibility, ABO incompatibility most common causes • Usually occurs with 2nd or later pregnancies • Requires maternal IgG antibodies and RBC antigens in fetus • can be prevented by administration of anti-Rh to Rh negative mothers after each pregnancy
Autoimmune HA • Occurs due to formation of autoantibodies that attack patient’s own RBC’s • Generally has 2 types: Warm & Cold each type is characterized by ability of autoantibodies to fix complement & site of RBC destruction • Often is secondary ,associated with either lymphoproliferative disease ,collagen vascular disease ,&infections.
Associated & leading causes-AIHA • SLE – due to immune dysregulation • Non-Hodgkins lymphomas • Hodgkins disease • Myeloma • HIV • Hepatitis C • Mumps , Mycoplasma infections • Idiopathic
Warm Type - AIHA • Mainly IgG antibodies • Fix complement to level of C1 & C3 • Antibodies are warm n bind best at a temp of 37 C. • Fc receptors +/- C3b recognized by macrophages, • Hemolysis primarily extravascular • About 60% is associated with other disorders. • Respond to steroids(prednisone 2mg/day) splenectomy in severe chronic cases.
Cold Type-AIHA • IgM mediated, most commonly with Mycoplasma infections • Antibodies can bind at 6º C or lower • Fix entire complement cascade • Typically only complement found on cells(Macrophages have no Rcs to detect IgM coated cells , if complement is absent. • Intravascular hemolysis (by hepatic cells) • 90% associated with other disorders. • Shows no response to steroids, splenectomy; responsive to plasmapheresis