Download
1 / 30
330 likes | 509 Views
Hemolytic anemia. Excessive destruction of red cells. Acute Hemolytic anemia. Chronic Hemolytic anemia. Congenita l. Acquired : Immune Non-immune. Classification of hemolytic anemia. - Intravascular hemolytic anemia :. - Turbolent and Marsch hemoglubinuria.

E N D
Hemolytic anemia Excessive destruction of red cells Acute Hemolytic anemia Chronic Hemolytic anemia Congenital Acquired : Immune Non-immune
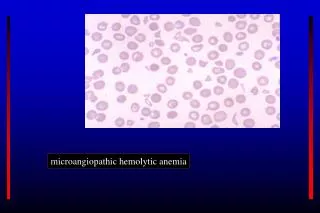
Classification of hemolytic anemia - Intravascular hemolytic anemia : - Turbolent and Marsch hemoglubinuria • Fibrin deposetion : DIC , TTP , UHS (Microangiopathic ) • Complement lysis : PNH , PCH , • and Non - compatible blood transfusion - Enzymppathies: G6PD D. , Pyrovate Kynase.d. - Toxin : colestidium velshay bacter - Extravascular hemolytic anemia RBC desruction by : - Immune Liver - Membran defect Spleen Other tissues
Laboratory Signs of Accelerated Red Cell Destruction - Decreased erythrocyt life span - Increased catabolism of heme. 1- Hemoglbinemia 2- Hemoglobinuria 3- Hemosiderinuria 4- Methemalbumineuria 5- Absent Haptoglobin 6- Reduced serum hemopexin level • Fall in blood hemoglobin level at a rate greater than • 1.0 g/dl/week
In the chronic hemolytic anemia • - quite severe anemia • can be tolerated with symptoms only arising on exercise. • -The patients jaundiced but this is oftenmild. • The urine is dark especially after standing • The spleen tend to be enlarged to degree of the underlying cause of the hemolysis . • - Leg ulcer usualy over the lateral malleolus
Immune-Mediated Hemolytic Disorders 1- IgG warm autoantibodies: IgG bind to RBC at 37c but fail to agglutinate the RBC. 2-Cold agglutinins: almost always are are of the IgM subtype and clump RBC at cold temperatures. 3- Donath-Landsteiner ( IgG) antibodies. Antibodies bind to RBC membranes in the cold and activate the Hemolyitic complement cascade .
Laboratory features of hemolytic anemia - Raised level of unconjugated bilirubin - Reticulocytosis - Urine hemosiderinuria - Red cell survival studies with C-labelled - Erythroide hyperplasia in bone marrow - Examination of peripheral blood smear - Direct antiglobulin test ( Coombs test ) - Absent haptoglubin - Hemoglubinemia and hemoglubinuria
The Antiglobulin ( Coombs” ) Test The test for routine detection of immunohemoiytic anemia , used most widely is the direct antiglobulin or Coombs” test. Positive results indicated thet the red cells are coated with IgG and / or complement components, especially C3. 2- 5 % of patients with immuno-hemolytic disease have negative test results because the amount of globulin on the cell surface is below the detection limits.
The Osmotic Fragility Test The Osmotic F.T. is a measure of the resistance of erythrocytes to hemolysis by osmotic stress . The test consists of exposing red celle to decreasing strengths of hypotonic saline Solutions and measuring the degree of hemolysis. Normally , hemolysis begin 0.45 to 0.50 g/dl and at which it is complete normally 0.30 to 0.33 g / dl. Increased fragility is indicated by a shift of the curve to the left or high value for median corpuscular fragility ( MCF ).
Chronic Congenital Hemolytic Anemia - Various degree of anemia - Jaundice - Crises - Splenomegaly - Cholelithiasis - Leg Ulcers - Skeletal Abnormalities
Hemoglubin defects • Defects of synthesis : • the thalassemias syndrome. - Defects of structure : Sickle cell disease.
Acute Hemolytic anemia Congenital Acquired : Immune Non-immune
Etiology of Hemolytic anemia 1- Congienital : Defect of Hemoglobin synthesisand structure Thalassemia Sickle cell disease Unstable hemoglobins Membrane defects Hereditary spherocytosis Hereditary elliptocytosis Red cell enzyme defects G6PD deficiency Pyruvate kinase deficiency 2- Acquired (Non-Immune) 3- Acquired ( immune )
Etiology of Warm –antibody type autoimmune Hemolytic A. Idiopatic (primary) Secondary : 1- Lymphoprolifrative diseasee, CLL ,NHL…. 2- Connective tissue diseases ,SLE,variable immunodeficiency 3- Immune deficiency disorders,AIDS, common variable imm.d. 4- Druges induced immuno-hemolytic anemia: penicilline , Quinidine , Methyldopa , Cephalosporine
Treatment of warm autoantibodu H.A. If mild ,no specific therapy may needed. Treatment of secondary causes ,underling diseases. When treat underling diseases Unsuccessful: - Folic acid and Vit B12 - RBC transfusions - Corticosteroids - Splenoctomy - IV immunoglobulin • Immunosupressive therapy - Danazol and Vinca alkaloids
Treatment of warm autoantibodu H.A. If mild ,no specific therapy may needed. Treatment of secondary causes ,underling diseases. When treat underling diseases Unsuccessful: - Folic acid and Vit B12 - RBC transfusions - Corticosteroids - Splenoctomy - IV immunoglobulin • Immunosupressive therapy - Danazol and Vinca alkaloids
- Folic acid and Vit B12 - RBC transfusions - Corticosteroids - Splenoctomy - IV immunoglobulin • Immunosupressive therapy - Danazol and Vinca alkaloids