Download
1 / 145
1.46k likes | 1.68k Views
Pulmonary Physiology:. Electron micrograph showing a pulmonary capillary (C) in the alveolar wall. Figure 4.02. Changes in cross-sectional area of airways through successive generations of branchings.

E N D
Electron micrograph showing a pulmonary capillary (C) in the alveolar wall.
Figure 4.02. Changes in cross-sectional area of airways through successive generations of branchings
The Pulmonary Tree with some blood vessels as seen in a "corrosion" preparation: 1 = trachea; 2 = left principal bronchus; 3 = right principal bronchus; 4 = aorta, 5 = thoracic aorta; 6,7,8 = bronchial arteries.
Scanning electron micrograph of a section of lung showing many alveoli and a small bronchiole
Lung Composition. Left: Percentages of liquids and solids on a weight basis; Right: Percentages of gas, liquids and solids on a volume basis
To understand how the values of the partial pressures of the three respiratory gases change from the point of inspiration, through the "respiratory compartments" - to the expiration point, including the FRC's buffer role.
Figure 1.01. Standard (static) lung volumes as measured with a spirometer
Figure 1.02. A Forced Ventilatory Capacity (FVC) recording on which the volumes expired at the end of 0.5, 1, 2 and 3 seconds are indicated (FEV0.5, FEV1.0, FEV2.0, FEV3.0).
Figure 1.03. An FVC recording on which the points of 200 ml and 1200 ml of expired volumes are indicated. The slope of the line between these 2 points is the average flow rate during this period (called the FEF0.2-1.2L).
Figure 1.04. An FVC recording on which the 25% and 75% points of the FVC have been indicated. The slope of the line between these 2 points is the average flow rate during this period (called the FEF25-75%). The same FVC maneuver is again used and the average flow rate during the middle 50% of the FVC is shown (i.e. between points where 25% and 75% of the FVC has been expired).
Figure 1.05. Changes in the gaseous partial pressures from inspiredatmospheric air to expired gas (in mmHg).
Figure 2.03. Changes in lung volume, air flow, intrapleural pressure, and alveolar pressure during normal (tidal) breathing. The dashed intrapleural pressure line would be followed if there were no airway resistance). The diagram at the left shows the lung and a spirometer measuring the changes
Figure 5.01. Effect on distribution of ventilation due to inspirationfrom FRC (panel A) vs. starting from RV (panel B).
Table 6.01. Comparison of pulmonary and systemic hemodynamic variables during rest and exercise of moderate severity in normal adult man.
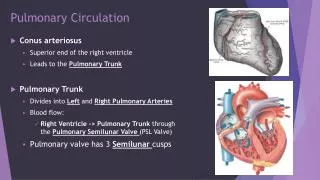
Figure 6.01. Pulmonary vs. systemic circulation pressures (mmHg).
This diagram shows the virtual matching of blood flow (FLOWS) and air flow (VOLUMES) within the normal lung.
Figure 6.02. Pulmonary vascular resistance (PVR) falls as the very compliant (distensible) vessels are subjected to higher distending pressures.
Table 6.02. Factors that when varied cause "passive" changes in pulmonary vascular resistance (PVR) and the direction of the responses.
Figure 6.06. Four zone model of pulmonary circulation in which hydrostatic arterial and venous pressures fall with increasing distances up the 30 cm height of the lung. (a=arterial, A=alveolar, V=venous.)
Table 6.03. Important causes of "active" changes in pulmonary vascular resistance (PVR) and the direction of the responses
Figure 7.01. Perfusion-limited (nitrous oxide = N2O & oxygen) transfer of oxygen vs. diffusion-limited transfer (carbon monoxide = CO).
Figure 7.06. Hemoglobin-oxygen association-dissociation curve at pH 7.4 and 37o C.
Figure 7.07. Changes in the Hb-oxygen association-dissociation curve with temperature, pH and 2-3 DPG.
Figure 7.08. Comparison of P80 of Quechua (Andes Mountains) inhabitants with Western Europeans (sea level) under normal conditions and after pH is lowered from 7.4 to 6.7. "Double effect" rightward shifts of Quechuas aids unloading of oxygen from blood to tissues.
Figure 7.09. Loading of CO2 from tissure to blood and associated O2 release from blood to tissue.
Figure 7.10. Showing the relative importance of the three ways in which CO2 is transported from the tissues to the lungs (right).
Figure 9.01. Characteristics of the four classical hypoxias compared with the normal state (see Table 9.01 for more details).
Table 9.01. Classification of the causes of hypoxia in terms of alveolar PO2, arterial P02, arterial oxygen content, venous P02, and venous oxygen content. The last column indicates whether increased inspired fractional oxygen will alleviate the problem
Figure 9.02. Comparison of the oxygen dissociation curves of normal blood, blood containing 20%, 40% and 60% carboxyhemoglobin (COHb), and blood from a severely anemic patient.
Figure 9.03. Increasing 2,3-diphosphoglyceric acid (DPG) concentration causes the hemoglobin-oxygen association-dissciation curve to shift to the right, ie. to decrease Hb's affinity for oxygen (P50 values are 15, 20, 27, 34, and 42 mm Hg from left to right).
Table 13.01. Mechanisms that contribute to the defense of the respiratory tract
Figure 13.01. Mechanisms of aerosol particle deposition include sedimentation via gravity, inertial impaction, and diffusion by Brownian motion
Table 13.03. Summary of the fate of circulating substances during a single passage through the intact pulmonary circulation.
The Respiratory System 1) Thelung ‑‑ two functional components: Airways (convection of gas) (p. 550-2, 499-502, 475-7, 480;Fig. 17-2) Alveoli (site of gas exchangeordiffusion; (also includes respiratory bronchioles and alveolar sacs) (p. 551,502, 477; Fig. 17-2)) 2) The pump muscles (p. 548, 500, 499-500, 476; Fig. 17-2a): Inspiratory: diaphragm, external intercostals, other accessory muscles when respiratory drive increases Expiratory: internal intercostals, abdominals; typically inactive at rest (in humans)
Consider flow from a tube at the bottom of a bucket: The higher the level of water in the bucket, the greater the pressure of the water at the bottom and, therefore, the greater the flow. Therefore, flow is proportional to the pressure gradient. The greater the resistance of the tube, the less the flow. Therefore, flow is inversely proportional to resistance. Flow = Δ P/R This is the most important equation you will need.
The pressure gradient and resistance determine flow R ΔP Hydraulic version of Ohm's law used to determine electric current flow through a circuit (see section related to membrane potential) and is identical to that used to describe blood flow (pp. 453-4, 408-10).
Flow to and from the alveoli depends on: a) the resistance (R) to flow offered by the airways (reflecting their size), and b) the pressure generated (ΔP) by the respiratory pump muscles.
Airway resistance: Depends on the physical properties of the fluid (air) and the geometry of the tubes (airways); given by Poiseuille's Law(p. 560, 513, 490): R = 8 η l /π r4 where: η = the density of the fluid l = the length of the tube r = the radius of the tube. r is the most important because it is raised to the fourth power.
Airway resistance is controlled: passively (lung volume, strength of airway wall) actively (degree of contraction of airway smooth muscle).
Control of airway smooth muscle tone • (the “R” in V = ΔP/R) • (p. 560-1, 513-4, 490-1) • Depends on: • sympathetic (dilator) and • parasympathetic (constrictor) • activity in branches of the autonomic nervous system. .
Sympathetic (dilator) effects can be: direct ‑‑ release of norepinephrine from sympathetic terminals into the ganglia containing the parasympathetic fibres, thereby reducing the level and/or effectiveness of parasympathetic activity, or indirect ‑‑ epinephrine released from the adrenal medulla into the circulation, causes relaxation of airway smooth muscle. Parasympathetic (constrictor) effects are: direct-- via release of acetylcholine from postganglionic fibres directly onto airway smooth muscle. Also depends on local levels of O2 andCO2 (p. R19-20 in notes; Fig. 17‑17 p 576-7, 519, 497)
. The “ΔP” in V = ΔP/R Barometric pressure, PB (p. 552, 503, 480) ‑‑ the "weight" of the atmosphere. Pressures are relative to PB at sea level, PB = 760 mmHg (or 1 ATA or 100 kPa or 1000 hPa or 1000 cmH2O) The local (ambient) PB is set equal to zero; all other pressures are relative to this value. Thus: pressures > PB are positive pressures < PB are negative Units:most respiratory physiologists and clinicians still use cmH2O. 1 mmHg = 13.6 mmH2O (mercury is 13.6 times as dense as water) = 1.36 cmH2O