Download
1 / 65
660 likes | 937 Views
Concussion Management: What is the Evidence?. Charles W. Webb, DO Assistant Professor Family Medicine & Orthopedics Director, Primary Care Sports Medicine Oregon Health & Science University Portland, OR. Objectives. What is concussion (mTBI)? Concussion Basics

E N D
Concussion Management: What is the Evidence? Charles W. Webb, DO Assistant Professor Family Medicine & Orthopedics Director, Primary Care Sports Medicine Oregon Health & Science University Portland, OR
Objectives • What is concussion (mTBI)? • Concussion Basics • What is the management of Concussion (mTBI)? • Concussion Evaluation • Acute Concussion Evaluation (ACE) • Role of Neuropsychological Testing • Concussion Treatment & Management • How do we determine recovery and return to play/duty? • Zurich Consensus Statement • CPG mTBI
What is Concussion? • Consensus from 1st and 3rd International Conference for Concussion • May be caused either by direct blow to the head, face, neck, or elsewhere on the body with an impulsive or rotational force transmitted to the head. • Typically results in the rapid onset of short-lived impairment of neurologic function that resolved spontaneously. • Results in neuropathic changes, but the acute clinical symptoms reflect a functional disturbance rather than structural injury. • Results in a graded set of clinical syndromes that may or may not involve loss of consciousness; resolution of the clinical and cognitive symptoms typically follow a sequential course • Typically associated with grossly normal structural neuroimaging. “Concussion” first used by Rhazes (850-923 AD) Defined as “abnormal physiologic state without gross traumatic lesions of the brain” > 1000 years later we use (essentially) the same definition
Concussions Not Just a Football Problem…. Injury rate per 1000 exposures • Football 0.44 • Girls soccer 0.35 • Girls basketball 0.24 • Boys soccer 0.23 • Wrestling 0.12 • Boys basketball 0.07 Most injuries occur in football players due to the large number of participants • .36/1000 in females • .22/1000 in males 40% higher in girls 240% in B-Ball
More Interesting Facts… • Head injury is the most frequent direct cause of death in sports • About 350,000 concussion per year in football • 95% are mild (simple) (Grade 1), 5% are the others • 8 Deaths per year • Acute SDH or SIS • 1000 serious brain injuries • 300,000 mTBI
Symptoms of Concussion • Headache • Nausea • Vomiting • Drowsiness • Numbness or tingling • Dizziness • Balance Problems • Sleeping more than usual • Difficulty concentrating • Difficulty remembering • Sensitivity to light • Sensitivity to noise • Feeling slowed down • Feeling as if “in fog” • Trouble falling asleep • More emotional than usual • Irritability • Sadness • Nervousness
Signs of Concussion • Cognitive: • Unawareness of period, opposition, game score, • Poor concentration • Confusion • Post Traumatic Amnesia • Retrograde • Antegrade • LOC • Repetitive questioning • Repetitive questioning • Repetitive questioning • Physical: • Poor coordination • Unstable gait • Seizure • Vomiting • Slurred speech • Inappropriate behavior or emotions • Vacant stare • Slow to respond
What is it Really? Altered cellular metabolism causes decreased blood flow to the brain at a time the brain needs it most The resulting “mismatch” increases the vulnerability of the brain to further injury. • Coup and countercoup forces lead to acceleration/ deceleration injury • Significant changes in cerebral glucose metabolism (GCS) • Neurometaboliccascade of reactions • Depolarization due to excitatory amino acid-mediated ionic fluxes across cell membranes, depletion of mitochondrial adenosine triphosphate (ATP), and alterations in vascular permeability • Alterations in blood flow?
500 Calcium 400 K+ 300 Glucose % of normal 200 Glutamate 100 50 2 6 12 20 30 6 24 3 6 10 0 Cerebral Blood Flow hours days minutes Neurometabolic Cascade FollowingTraumatic Brain Injury (Giza & Hovda, 2001) Giza et al, The Neurometabolic Cascade of Concussion. J Athl Train. 2001 Jul–Sep; 36(3): 228–235.
Why are we Concerned? • Traumatic brain injury is a common and potentially life-threatening injury • Possible long-term sequelae and disability • Important interventions prior to injury • Return-to-play decisions are often left to the primary care provider http://www.cnn.com/2010/HEALTH/02/03/concussions.teen.brains/index.html?iref=allsearch
“Real” Statements • “The ED staff told me that I couldn’t play for 3 weeks because I had a concussion. Why 3 weeks?” • The ED physician told my son he could return to the ice in 72 hours.” • “My pediatrician asked me if my child had lost consciousness. I replied ‘No.’ He told me just to watch her.” • “The main concern or worry with TBI is loss of consciousness, right?” • “My teacher must not believe that I have had a concussion because I am not getting any of the help that my doctors have recommended.”
Grading • Concussion is defined as the transient impairment in neurologic function secondary to trauma. • Incidence increases as the sport and behavior becomes increasingly violent and aggressive. • “Second Impact Syndrome” results from repeated concussions and is associated with fatal outcomes • Grade 1: • No LOC • Confusion w/o amnesia • Resolves in < 15 mins. • Grade 2: • No LOC • Confusion w/ amnesia • Symptoms > 15 mins. • Grade 3: • LOC (any) Quality Standards Subcommittee, American Academy of Neurology. Practice parameter The management of concussions in sports. Neurology 1997;48:581-5.
British Journal of Sports Medicine 2009 43 (Suppl I) i76-i84.
Zurich Concussion in Sports Consensus Statement • Abandon the simple vs. complex terminology • Difference between children & adolescents • Concussion evaluation • Sideline • Follow up clinical evaluation • Neuropsychological testing • Return to play guidance
Management • Sideline evaluation • Medic Evaluation • SCAT 2 • Imaging • X-ray, CT, MRI, fMRI, MSI, PET, SPECT • Neuropsychological testing • Balance Testing • Education • Neurocognitive Rehabilitation • Pharmacology • Amitriptyline • Corticosteroids • Anitoxidants • NSAIDS • Calcium Channel Blockers • Vit B3 • Hyperbaric Oxygen • Methylphenidate • Sertraline Multifactorial Approach McCrory P, Meeuwisse W, Johnston K, et al. Consensus statement on concussion in sport, Zurich, November 2008. Clin J Sport Med. 209; 19: 185-200.
Sideline Evaluation • Symptom Assessment • Neurological Examination • Cognitive Testing • Balance Error Scoring System (BESS) Rieman BL, Guskiewics K. Effects of mild head injury on postural stability as measured through clinical balance testing. J. Athl. Train. 2000; 35:19-25. Eckner J, Kutcher J. Concussion symptom scales and sideline assessment tools: A clinical literature update. Curr Sports Med Rep. 9; 1:8-15, 2010.
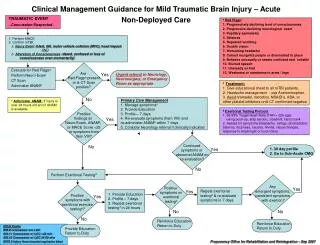
Initial Management in Deployed Setting Traumatic Event occurs AOC/LOC Admin MACE Assess for red flags and Sx’s Red Flags Progressively declining LOC Progressive declining neuro exam Pupil asymmetry Seizures Repeated vomiting Clinician verified GCS <15 Neruo deficit (motor or sensory) LOC >5 min Double vision Worsening HA Cannot rec people Slurred speech Weakness PCM educational sheet to all mTBI pts Reduce stiimulus environments Rest Aggressive HA management Avoid tramadol, narcotics Consider nortriptyline or amitripyline Implement duty restrictions Send consult to tbi.consult@us.army.mil for further guidance Consider evac to higher LOC Document concussion in EMR Refer to Level 3 Red Flags? Primary Care Mgmt Re-eval q 1-3d up to 7d Sx’s or MACE <25 Symptoms Resolve Symptoms Confusion <24° Unusual behavior Irritability Unsteady on feet Vertigo/ Dizziness HA Photophobia Phonophobia Perform exertional testing Alt MACE Continue PCM Screen for depression Combat Stress Exertional Testing Protocol 65-85% Max HR using push-up, step aerobic, treadmill, hand crank Assess for sx’s or MACE <25 Positive sx’s MACE <25 Continue concussion and combat stress mgmt up to 14d Refer to level 3 Educate and RTD RTD: neurocog test if avail and expertise for interpretation
To Image or Not to Image • Is it helpful? • Not essential for simple concussive injury • The injury is at the cellular level • Prevalence of CT scan abnormalities • 5% among patients with a GCS = 15, and 30% for those presenting with a GCS = 13 • 1%incidence of abnormalities leading to neurosurgical intervention Bazarian J, Blyth B, Cimpello L. Bench to bedside: Evidence for brain injury after concussion – looking beyond the computed tomography scan. Acad Emerg Med 2006; 13:199-214.
When is Imaging Recommended? • Consider urgent imaging if suspicion of intracerebral lesion: • prolonged unconsciousness • persistent mental status alterations • abnormalities on neurologic examination • worsening symptoms
Neuroimaging in the Acutely • CT vs. MRI • In case series of patients with mild TBI, MRI abnormalities were reported in 30 percent of cases with normal CT findings • Most of these additional abnormalities were lesions "consistent with axonal injury." • CT is the imaging of choice in the E.D. • MRI may be more useful in evaluation of chronic sequelae Mendez CV, Hurley RA, Lassonde M et al. Mild traumatic brain injury: neuroimaging of sports related concussion. J Neuropsychiatry Clin Neurosci 2005; 17(3):320-335.
Evidence for Neuroimaging • Level A: noncontrast head CT • loss of consciousness • posttraumatic amnesia • headache, vomiting age older than 60 years • drug or alcohol intoxication posttraumatic seizure • deficits in short-term memory GCS score less than 15 • focal neurologic deficit coagulopathy • physical evidence of trauma above the clavicle • Level B: noncontrast head CT • no loss of consciousness • posttraumatic amnesia • focal neurologic deficit vomiting, • severe headache age 65 years or older • physical signs of a basilar skull fracture GCS score less than 15 • Coagulopathy • dangerous mechanism of injury American College of Emergency Physicians Clinical Policy on Neuroimaging in the ER, DEC 2008; http://www.acep.org/acepnews.aspx?id=45443
Neuropsychological Testing Evidence in college and professional athletes recovery patterns last from several hours to up to 7 days. Considered the Gold Standard in concussion assessment Not validated in concussed athletes No consensus in which test is most sensitive Recommended as a way to track progress to recovery • Pencil and Paper • Trail making • Digit symbol substitution • Controlled oral work association • Time consuming, not portable, hard to do on the sideline • Computer • Automated neuropsychological assessment metrics (ANAM) • Cogsport • Headminder • Immediate Post-Assessment of Concussion Test (ImPACT) Collie A, makdissi M, Maruff P, et al. Cognition in the days following concussion comparison of symptomatic versus asymptomatic athletes. J Neurol Neurosurg Psychiatr 2006; 77:241-245.
ImPACT MEMORY COMPOSITEControl vs. Concussed Athletes Significant difference between groups out to at least 8 days post-injury N.S. p.<.00001 p.<.0001 p.<.03 N=410 . *Lower score indicates poorer performance Collins MW, Lovell MR, Maroon et al. Medicine and Science in Sports Exercise, 34:5;2002
N.S. p.<.005 p.<.0004 N.S. ImPACT REACTION TIME COMPOSITEControl vs. Concussed Athletes Significant difference between groups out to 5 days post-injury N=410 . *Higher score indicates poorer performance Lovell MR, Collins MW, Maroon et al. Medicine and Science in Sports Exercise, 34:5;2002
Balance Testing • Somatosensory aspects function normally • Integration b/t visual & vestibular components does not function normally • Neurocom Sensory Organization Test • Uses a force plate (forces and angles ankle, knee, hip) not portable, expensive • Balance Error Scoring System (BESS) • Objective tool with minimal cost and training • SCAT 2 • Can have postural deficits after symptom resolution Guskiewics KM, Ross SE, Marshall SW. Postural stability and neuropsychological deficits after concussion in colligate athletes. J Athl Train 2001;36(3):263-273.
Treatment Options • What is out there? • No Specific Medical Therapies for concussion. • No RCT’s esp double blinded • No magic pill to make it go away • Most patients improve with education, cognitive rest and time for the brain to recover
Treatment Options • Cognitive and Physical REST • Educational interventions • Neurocognitive rehabilitation • Pharmacological Interventions
Sports ConcussionA Few Facts • Some Injuries are worse than others. • Some athletes are more vulnerable • Pre-injury risk factors combine with injury (modifiers) • # previous concussions, headache, ADHD, LD, mood • Other possible factors that influence recovery • Magnitude of force that is received • Location that force is received • Defensive position/ prep of individual receiving force • Size, speed factors
Recovery From Concussion:How Long Does it Take? WEEK 5 WEEK 4 WEEK 1 WEEK 3 WEEK 2 N=134 High School athletes Collins et al., 2006, Neurosurgery
Zurich CIS Consensus • “Cornerstone” is Physical & Cognitive Rest • Graduated RTP: When asymptomatic at rest • Stepwise progression, proceed to next level if asymptomatic at current • Each step takes 24 hours; approximately 1 week to fully RTP • Same day RTP: not appropriate in child or adolescent (possible in adults ONLY if in a well established system)
Keys to Recovery Resting the brain & getting good sleep No additional forces to head / brain Managing / facilitating physiological recovery Avoid activities that produce symptoms Not over-exerting body or brain Ways to over-exert Physical Emotional Cognitive! (concentration, learning, memory)
Exertional Effects • Increase or re-emergence of post-concussion symptoms following significant exertional activity • Physical activity • Cognitive activity • No prolonged concentration • No prolonged homework • No prolonged classes (block scheduling) • No Prolonged days
Educational Intervention • Early patient education has the strongest evidence • Symptom related education • Reassurance that cognitive rest and time King NS, Crawford S, Wendon FJ, et al. Interventions and service need following mild and moderate head injury: the Oxford Head Injury Service. Clin Rehabil 1997; 11:13-27. Miittenberg W, Canyock EM, Condit D, et al. Treatment of post-concussive syndrome following mild head injury. J Clin Exp Neuropsychol 2001;23:829-836.
Neurocognitive Rehabilitation • Focus on treating specific individualized cognitive deficits • Most widely used treatment for severe brain injury • No conclusive evidence supporting improved outcomes in mTBI • Min Improvement in neuropsychological testing (Practice effect?) -Comper P, Bisschop SM, Carnide N, et al. A systematic review of treatments for mild traumatic brain injury. Brain Inj 19;11 863-880, 2005 -Elgmark A, Emanuelson I, Bjorklund R, et al. Mild traumatic brain injuries: the impact of early intervention on late sequelae. A randomized controlled trial. Acta Neurochirurgica. 149;2:151-160, 2007. -Ghaffar O, McCullagh S, Ouchterlony D, et al. Randomized treatment trial in mild traumatic brain injury. J Psychosomatic Research, 61;2:153-160, 2006.
Pharmacology Treatment • Appropriate in two situations: • Management of specific symptoms • Sleep disturbance, anxiety, etc. • Modification of the underlying pathophysiology to affect duration of symptoms
Pharmacology • The most common SX for which TX is indicated is the post-concussive headache • A recent systematic review of pharm interventions after mTBI failed to produce solid evidence that any specific drug treatment is effective for one or more symptoms Comper P, Bisschop SM, Carnide N, et al. A systematic review of treatments for mild traumatic brain injury. Brain Inj 2005; 19(11): 863-880.
Amitriptyline • Conflicting evidence as treatment for persistent PCHA. • 1 Case series found 75-225mg/d helps HA • RCT found no benefit Saran A. Antidepressants not effective in headache associated with minor closed head injury. Int J Psychiatry Med 1988;18:75-83. Tyler GS, McNeely HE, Dick ML. Treatment of post-traumatic headache with amitryptiline. Headache 1980;20:213-216.
Corticosteroids • Used to reduce inflammation and stabilize cell membranes • Systematic review of RCT’s in Acute brain injury demonstrated considerable uncertainty Albertson P, Roberts I. Corticosteroids in acute brain injury: systemic review of randomized controlled trials. BMJ 1997:314:1855.
Antioxidants • Numerous beneficial and protective effects in animal models involving physical, cognitive and affective issues • No human trials have demonstrated efficacy • Recent concern in epidemiologic studies on CVD found that antioxidant use increased cancer incidence Rigg JL, Elovic EP, Greewald BD. A review of the effectiveness of antioxidant therapy to reduce neuronal damage in acute traumatic brain injury. J Head Trauma Rehabil 2005; 20(4):389-391.
NSAIDS • Arachidonic Acid Metabolites thought to exacerbate central nervous system injury • Cyclooxygenase inhibitors (Ibuprofen) and mixed cyclooxygenase-lipoxygenase inhibitors (indomethacin) have shown some benefit in animals with spinal injury • No specific studies have been done in human mTBI Hallnebeck J, Jacobs T, Faden A. combined PGI2, indomethacin and heparin improves neurological recovery after spinal trauma in cats. J Neurosurg 1983;58:749-754.
Calcium Channel Antagonist • Calcium influx through voltage channels may contribute to secondary brain injury • Multiple RCT’s have not shown benefit in improved outcomes • May be a thought for future research as these studies only looked at peripheral acting agents. -Teasdale G. A randomized trial of nimodipine in severe head injury. J Neurotrauma 1991;9:S545-550. -Compton J, Lee T, Jones N. A double blinded placebo controlled trial of the calcium entry blocking drug nicardipine in the treatment of vasospasm following severe head injury. Br J Nerosurg 1990;4:9-16.
Nicotinamide (Vit B 3) • Potent Neuro-protectant following brain injury in animals • Shown to speed recovery in Rats • No studies have been able to translate this to humans -Hoane M, Akstulewics S, Toppen J. Treatment with vitamin B3 improves functional recover and reduces GFAP expression following traumatic brain injury in the rat. J Neurotruama 2003;20(11):1189-1199.
Hyperbaric Oxygen • May enhance cerebral oxygenation • Thereby enhance injury recovery post concussion • MOA is cerebral vascular constriction • Improved glucose metabolism • Decreased cerebral edema • May harm by increasing oxygen supply for free radical reactions • In randomized trials HBO improved overall mortality, but not functional improvement at 12 months Rockswold G, Ford S, Anderson D. Results of a prospective randomized trial for the treatment of severely brain injured patients with hyperbaric oxygen. Neurosurgery 1992;76:929-934.
Methylphenidate • Significant decrease in depressive symptoms • Minimal improvement in cognitive function recovery compared to placebo • 20mg/day • No increase in daytime sleepiness • 4 week end point Lee H, Jim S, Kim J, Et al. Comparing effects of methylphenidate, sertraline, and placebo on neuropsychiatric sequelae in patients with traumatic brain injury. Human Psychopharm 20;2:97-104, 2005.