Download
1 / 30
300 likes | 533 Views
IMMUNE DISORDERS – EXAGGERATED RESPONSE; DAMAGE HOST TYPE I – ANAPHYLAXIX, ALLERGY LOCALIZED, SYSTEMIC TYPE II- CYTOTOXIC REACTIONS ABO BLOOD GROUPS TRANSFUSION REACTION HEMOLYTIC DISEASE – NEWBORN TYPE III- IMMUNE COMPLEXES TYPE IV- DELAYED - CMI

E N D
IMMUNE DISORDERS – EXAGGERATED RESPONSE; DAMAGE HOST TYPE I – ANAPHYLAXIX, ALLERGY LOCALIZED, SYSTEMIC TYPE II- CYTOTOXIC REACTIONS ABO BLOOD GROUPS TRANSFUSION REACTION HEMOLYTIC DISEASE – NEWBORN TYPE III- IMMUNE COMPLEXES TYPE IV- DELAYED - CMI POISON IVY, CONTACT DERMATITIS AUTOIMMUNE DISEASES TRANSPLANT REJECTION – HOST VS GRAFT, GRAFT VS HOST
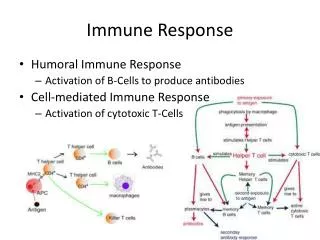
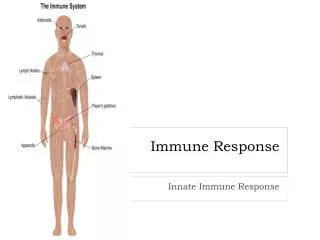
IMMUNE DISORDERS EXAGGERATED RESPONSE TO SECOND OR SUBSEQUENT EXPOSURE TO ANTIGEN WHICH RESULTS IN TISSUE DAMAGE IMMEDIATE (SECONDS TO MINUTES) – HUMORAL ANTIBODIES DELAYED (1-2 DAYS) – CMI REACTIONS TYPE I – ANAPHYLAXIS, ALLERGY INITIAL EXPOSURE – IgE SYNTHESIS, BINDS TO RECEPTORS ON BASOPHILS, EOSINOPHILS, MAST CELLS MAST CELLS – WHITE BLOOD CELLS – TISSUE LOCALIZED- PRODUCE VASOACTIVE MOLECULES (HISTAMINE) STORED IN VACUOLES NEAR MEMBRANE, HAVE RECEPTORS FOR IgE IgE BINDING SENSITIZES THESE CELLS TO THE ANTIGEN WHICH STIMULATED THE IgE SYNTHESIS
TYPE I – ANAPHYLAXIS - CONTINUED SECOND OR LATER ANTIGEN EXPOSURE ANTIGEN BINDS SPECIFIC ANTIBODY IgEON MAST CELLS, BASOPHILS, EOSINOPHIL TRIGGERS DEGRANULATION – RELEASE OF HISTAMINE, VASOACTIVE MOLECULES, PROTEASES SMOOTH MUSCLE CONTRACTION, VASODILATION, INCREASED VASCULAR PERMEABILITY, MUCUS SECRECTION = ANAPHYLAXIS
TYPE I ANAPHYLAXIS - CONTINUED • LOCALIZED– ATOPIC (OUT OF PLACE) • UPPER RESPIRATORY TRACT – SENSITIZED MAST CELLS IN MUCOUS MEMBRANES CAUSES: POLLEN SPORES, DANDER, HOUSE MITES SYMPTOMS: ITCHING, WATERY EYES, CONGESTION, SNEEZING, COUGHING TREATMENT: ANTI-HISTAMINE 2. LOWER RESPIRATORY TRACT - SAME ALLERGENS AIR SACS – ALVEOLI – DISTENDED, FLUID, MUCUS, ASTHMA 3.DIGESTIVE SYSTEM – HIVES RED SKIN GASTROENTERITIS
HUMAN BLOOD CELL DEVELOPMENT
TYPE I HYPERSENSITIVITY (ALLERGIC RESPONSE)
SKIN TESTING FOR CAUSE OF HYPERSENSITIVITY
TYPE I - ANAPHYLAXIS -CONTINUED • SYSTEMIC– GENERALIZED RESPONSE, WHOLE BODY RESPIRATORY IMPAIRMENT (SMOOTH MUSCLE CONTRACTION IN BRONCHIOLES) DROP IN BLOOD PRESSURE – ARTERIOLES EXPAND, BECOME MORE PERMEABLE, RAPID FLOW INTO TISSUE SPACES REDUCED VENOUS BLOOD RETURN, ASPHYXIATION, SHOCK RAPID, SEVERE, CAN BE FATAL CAUSES: DRUGS (E.G., PENICILLIN); INSECT VENOM (BEE); PEANUTS, ANTI-SERA (E.G., TETANUS ANTSERUM)
TYPE II HYPERSENSITIVITY CYTOTOXIC REACTIONS ANTIGEN-ANTIBODY REACTION DAMAGES (LYSES, KILLS) CELLS, RESULTS IN INJURY IgG, OR IgMREACT WITH CELL SURFACES, TISSUES FOREIGN IgG (INCOMING) REACT WITH HOST CELLS HOST IgG REACTS WITH FOREIGN CELLS (INCOMING) BLOOD TRANSFUSIONS WITH MISMATCHED BLOOD; ERYTHROBLASTOSIS FETALIS – HEMOLYTIC DISEASE OF NEW BORN
ABO BLOOD GROUPS PRODUCED RBC TYPE ANTIGENS ON RBC FROM GENE: AA IA BB IB AB A AND B IA & IB O NONE I POSSIBLE GROUP GENOTYPES AIAIA OR IAi BIBIB OR IBi A B IA IB O ii
ABO ANTIGENS & ANTIBODIES RBC TYPE ANTIGENS ON RBC ANTIBODIES IN BLOOD A A ANTI B B B ANTI A AB A AND B NEITHER O NONE ANTI A AND ANTI B
COMPLEMENT ACTIVATED- HEMOLYSIS IMMUNOHEMATOLOGY
TRANSFUSION REACTIONS RECIPIENT BLOOD CONTAINS ANTIBODIES (NATURAL); E.G., ANTI-B RECEIVES BLOOD WITH RBCs COATED WITH, E.G., ANTIGEN B INCOMING RBC HEMAGGLUTINATE, LYSE, CHILLS, FEVER, PROSTRATION, SHOCK, DEATH PREVENT BY BLOOD TYPING AND CROSS MATCHING BLOODS TYPING UNKNOWN BLOOD PLUS KNOWN ANTI A > CLUMP MEANS A TYPE ANTI B > B TYPE CLUMPING WITH BOTH ANTI A AND ANTI B > AB TYPE CLUMPING NEITHER A NOR B O TYPE
CROSS MATCHING BLOODS • MAJOR RECIPIENT SERUM PLUS DONOR RBC > IF AGGLUTINATION OCCURS THE DONOR RBC WOULD BE COATED BY RECIPIENT ANTIBODIES CIRCULATING IN BLOOD > CYTOTOXIC • MINOR RECIPIENT RBC PLUS DONOR SERUM > IF AGGLUTINATION OCCURS THIS BLOOD SHOULD NOT BE USED, BUT THIS IS NOT SO IMPORTANT AS THE MAJOR CROSS MATCH – INCOMING SERUM (CONTAINING SOLUBLE ANTIBODIES) WILL BE DILUTED IN RECIPIENT’S BLOOD, REDUCING THE SEVERITY OF THE PROBLEM • UNIVERSAL DONOR - TYPE O PERSON - THE ANTI A AND ANTI B ANTIBODIES WILL BE DILUTED IN RECIPIENT BLOOD; CAN BE USED FOR TYPE A, B, AB AND O RECIPIENTS • UNIVERSAL RECIPIENT - TYPE AB PERSON – NO ANTIBODIES TO REACT WITH INCOMING A, B, OR O CELLS
HEMOLYTIC DISEASE OF NEWBORN ERYTHROBLASTOSIS FETALIS Rh+ ANTIGENS ON SOME RBC RHESUS MONKEY RBC > RABBITS > ANTISERUM AGGLUTINATED MONKEY RBC, BUT ALSO AGGLUTINATED RBC OF SOME (BUT NOT ALL) HUMANS? SOME PEOPLE PRODUCE THE SAME ANTIGEN ON THEIR RBC AS DO RHESUS MONKEYS = RH+ INDIVIDUAL = 85% RH- INDIVIDUALS NO SUCH ANTIGEN AND NO ANTI Rh ANTIBODIES
HEMOLYTIC DISEASE OF NEWBORN • Rh- MOTHER, Rh+ FATHER (Rh+ IS DOMINANT) • FIRST OR LATER PREGNANCY WITH Rh+ FETUS, • SMALL HEMORRHAGES, BABY RBCs ENTER MOTHER’S BLOOD, SHE SYNTHESIZES ANTI Rh ANTIBODIES - NO PROBLEM • SECOND OR LATER PREGNANCY WITH Rh+ BABY MOTHER’S ANTI-Rh ANTIBODIES CROSS PLACENTA REACT WITH BABY’S RBC, LYSE, LACK OF OXYGEN HEMOGLOBIN RELEASED > DEGRADED TO BILIRUBIN (TOXIC) • IN UTERUS – OXYGEN FROM MOTHER, MOTHER’S LIVER PROCESSES EXCESS BILIRUBIN • BIRTH – LACK OF OXYGEN, BILIRUBIN IS NOT PROCESSED IN INFANT LIVER, BRAIN DAMAGE
HEMOLYTIC DISEASE OF NEWBORN MANAGEMENT • MONITOR MOTHER’S ANTI Rh ANTIBODY LEVEL DURING PREGNANCY TO CHECK FOR TITER INCREASE • FLUORESCENT LIGHT TO HELP BILIRUBIN BREAKDOWN • MONITOR BILIRUBIN LEVEL – DANGEROUS LEVEL – BLOOD EXCHANGE, Rh- BLOOD, 10 ML IN / 10 ML 0UT • SEVERE CASES - DETERMINE BILIRUBIN LEVEL AMNIOTIC FLUID - AMNIOCENTESIS INFUSION IN UTERO Rh- RBC INJECTED INTO FETUS ABDOMEN > LIVER, SPLEEN, FUNCTION FOR NEWBORN
HEMOLYTIC DISEASE OF NEW BORN PREVENTION GIVE EXPECTANT MOTHER ANTI-Rh ANTIBODY PREVENTS Rh+ RBC (BABY) FROM STIMULATING ANTI Rh ANTIBODY SYNTHESIS BY MOTHER RhoGamIgG FROM HUMANS; KNOWN TO CONTAIN ANTI-Rh ANTIBODIES REDUCES RISK FROM ~15% (UNTREATED) TO <0.1%
TYPE III – IMMUNE COMPLEXES DAMAGE HOST SMALL AG-AB COMPLEXES ESCAPE PHAGOCYTOSIS CIRCULATING COMPLEXES LODGE IN TISSUES – INFLAMMATION; PHAGOCYTES ARRIVE, CANNOT ENGULF THE SMALL COMPLEXES, RELEASE DIGESTIVE ENZYMES INTO TISSUES, FURTHER INJURY ACUTE POST-STREPTOCOCCAL GLOMERULONEPHRITIS INFLAMMATION OF THE GLOMERULI – BASEMENT MEMBRANE OF KIDNEY (BLOOD FILTRATION) ARTHRITIS - JOINT INFLAMMATION – ONE OF >100 CONDITIONS CALLED ARHTRITIS SYSTEMIC LUPUS ERYTHEMATOSUS – ARTHRITIS, VASCULITIS, GLOMERULONEPHRITIS
TYPE III HYPERSENSITIVITY
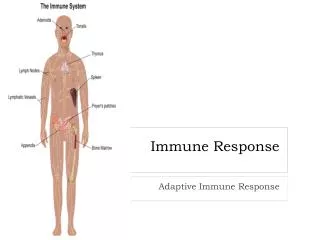
TYPE IV – DELAYED CMI REACTION SPECIFIC TH AND CTL CELLS - 24-48 HRS CELLS MIGRATE TO ANTIGEN (ON SECOND OR SUBSEQUENT EXPOSURE), DAMAGE HOST FIRST EXPOSURE – ANTIGEN STIMULATES CMI RESPONSE SECOND EXPOSURE – ANTIGEN FRAGMENTS PRESENTED ON CELL SURFACES; T HELPER AND CTLs ATTRACTED, DAMAGE CELLS, CYTOKINES INCREASE VASCULAR PERMEABILITY, ATTRACT OTHE LEUCOCYTES, EXACERBATE INFLAMMATION
TYPE IV – DELAYED CMI REACTION TUBERCULIN SKIN TEST FOR TB – (TUBERCULIN = M. TUBERCULOSIS PROTEIN AND ONE OF ITS ANTIGENS) PEOPLE INFECTED BY M. TUBERCULOSIS OR GIVEN BCG VACCINE: FORM CMI TO BCG (AND TUBERCLIN) INJECT TUBERCULI INTO SKIN: UN-INFECTED PERSON –– NO REACTION ANYONE PREVIOUSLY INFECTED OR VACCINATED WITH BCG INFLAMMATION AROUND SITE OF INJECTION EVIDENCE OF PREVIOUS OR ACTIVE INFECTION
AUTOIMMUNE DISEASES SELF-REACTIVE T AND B CELLS DAMAGE HOST HYPERSENSITIVITY TO ONE’S OWN SELF RHEUMATIC FEVER – ANTIODIES TO S. PYOGENES PILI EPITOPE CROSS REACT WITH HEART TISSUE – TYPE II HYPERSENSITIVIY TYPE I DIABETES – CYTOTOXIC T CELLS FORM AFTER INFECTION BY SOME VIRUS (?) & ATTACK AND DESTROY INSULIN- PRODUCING ISLET CELLS OF PANCREAS TYPE IV HYPERSENSITIVITY MULTIPLE SCLEROSIS - CMI ATTACKS MYELIN, DEMYELINATES AXONS, LOSS OF NERVE INSULATION AND FUNCTION