Download
1 / 30
310 likes | 652 Views
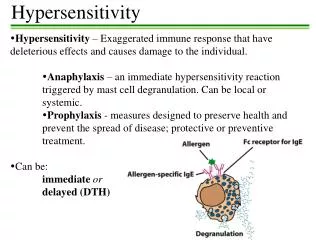
Lecture 21 Hypersensitivity Types II-V. Type II: Cytotoxic (ITH) Type III: Toxic Complex (ITH) Type IV: T Cell-Mediated (DTH) Type V: Stimulatory. Cytotoxic Hypersensitivity (Type II). Characteristics of Cytotoxic Hypersensitivity . Directed against cell surface or tissue antigen

E N D
Lecture 21Hypersensitivity Types II-V • Type II: Cytotoxic (ITH) • Type III: Toxic Complex (ITH) • Type IV: T Cell-Mediated (DTH) • Type V: Stimulatory
Characteristics of Cytotoxic Hypersensitivity • Directed against cell surface or tissue antigen • Characterized by complement cascade activation and various effector cells
Complement • Formation of membrane attack complex (lytic enzymes) • Activated C3 forms opsonin recognized by phagocytes • Formation of chemotactic factors • Effector cells possess Fc and complement receptors • macrophages/monocytes • neutrophils • NK cells
Examples of Type II Hypersensitivity • Blood transfusion reactions • Hemolytic disease of the newborn (Rh disease) • Autoimmune hemolytic anemias • Drug reactions • Drug-induced loss of self-tolerance • Hyperacute graft rejection • Myasthenia gravis (acetylcholine receptor) • Sensitivity to tissue antigens
ABO Blood Group Antigens A NAG Gal NAcGA Fuc H A antigen NAG Gal NAG Gal B antigen Fuc Precursor oligosaccharide H antigen Gal Gal NAG NAcGA (N-acetylgalactoseamine) Gal (galactose) B Fuc
ABO Blood Group Reactivity blood group genotypes antigens antibodies to (phenotype) ABO in serum A AA, AO A anti-B B BB, BO B anti-A AB AB A and B none O OO H anti-A/B
Hemolytic Disease of the Newborn first birth post partum subsequent RhD negative mother anti-RhD RhD positive red cells B cell Lysis Of RBC’s RhD positive fetus RhD positive fetus anti-RhD
Drug-Induced Reactions:Adherence to Blood Components blood cell adsorbed drug or antigen drug metabolite antibody to drug complement lysis
Diseases associated with immune complexes • Persistent infection • microbial antigens • deposition of immune complexes in kidneys • Autoimmunity • self antigens • deposition of immune complexes in kidneys, joints, arteries and skin • Extrinsic factors • environmental antigens • deposition of immune complexes in lungs
Inflammatory Mechanisms in Type III • Complement activation • anaphylatoxins • Chemotactic factors • Neutrophils attracted • difficult to phagocytize tissue-trapped complexes • frustrated phagocytosis leads to tissue damage
Disease Models • Serum sickness • Arthus reaction
Manifestations of T-Cell Mediated Hypersensitivity • Allergic reactions to bacteria, viruses and fungi • Contact dermatitis due to chemicals • Rejection of tissue transplants
General Characteristics of DTH • An exaggerated interaction between antigen and normal CMI-mechanisms • Requires prior priming to antigen • Memory T-cells recognize antigen together with class II MHC molecules on antigen-presenting cells • Blast transformation and proliferation • Stimulated T-cells release soluble factors (cytokines) • Cytokines • attract and activate macrophages and/or eosinophils • help cytotoxic T-cells become killer cells, which cause tissue damage
Types of Delayed Hypersensitivity Delayed Reaction maximal reaction time Jones-Mote 24 hours Contact 48-72 hours tuberculin 48-72 hours granulomatous at least 14 days
Jones-Mote Hypersensitivity • Now referred to as “cutaneous basophil hypersensitivity” • Basophils are prominent as secondary infiltrating cells. • Basophilic infiltration of area under epidermis • Induced by soluble (weak) antigens • Transient dermal response • Prominent in reactions to viral antigens, in contact reactions, skin allograft rejections, reactions to tumor cells and in some cases of hypersensitivity pneumonitis (allergic alveolitis) • May be important in rejection of blood-feeding ticks on the skin surface
Contact Hypersensitivity • Usually maximal at 48 hours • Predominantly an epidermal reaction • Langerhans cells are the antigen presenting cells • a dendritic antigen presenting cell • carry antigen to lymph nodes draining skin • Associated with hapten-induced eczema • nickel salts in jewellry • picryl chloride • acrylates • p-Phenylene diamine in hair dyes • chromates • chemicals in rubber • poison ivy (urushiol)
Tuberculin Hypersensitivity • Maximum at 48-72 hours • Inflitration of lesion with mononuclear cells • First described as a reaction to the lipoprotein antigen of tubercle bacillus • Responsible for lesions associated with bacterial allergy • cavitation, caseation, general toxemia seen in TB • May progress to granulomatous reaction in unresolved infection
Granulomatous Hypersensitivity • Clinically, the most important form of DTH, since it causes many of the pathological effects in diseases which involve T cell-mediated immunity • Maximal at 14 days • Continual release of cytokines • Leads to accumulation of large numbers of macrophages • Granulomas can also arise from persistence of “indigestible” antigen such as talc (absence of lymphocytes in lesion)
Epitheloid Cell Granuloma Formation • Large flattened cells with increased endoplasmic reticulum • Multinucleate giant cells with little ER • May see necrosis • Damage due to killer T-cells recognizing antigen-coated macrophages, cytokine-activated macrophages • Attempt by the body to wall-off site of persistent infection
Examples of Microbial-Induced DTH • Viruses (destructive skin rashes) • smallpox • measles • herpes simplex • Fungi • candidiasis • dematomycosis • coccidioidomycosis • histoplasmosis • Parasites (against enzymes from the eggs lodged in liver) • leishmaniasis • schistosomiasis
Type V Stimulatory Hypersensitivity • Interaction of autoantibodies with cellular receptors • Antibody binding mimics receptor-ligand interaction • Examples • thyroid stimulating antibody (mimics thyroid stimulating hormone [TSH] of pituitary binds to thyroid cell receptor • activation of B-cell by anti-immunoglobulin
Innate Hypersensitivity Reactions • Toxic shock syndrome (S. aureus TSS toxin) • hypotension, hypoxia, oliguria and microvascular abnormalities • excessive release of TNF, IL-1, IL-6 • intravascular activation of complement • Septicemia - Septic Shock • primarily due to lipopolysaccharide • Adult respiratory distress syndrome • overwhelming accumulation of neutrophils in lung • Platelet aggregation/adherence to macrophages by gram-positive bacteria • Superantigens • Gram positive enterotoxins • react directly with T-cell receptors and induce massive cytokine release