Download

1 / 1
10 likes | 158 Views
No. 032. Vasculitic Infarction of the testis – Is organ sparing possible?. David Pan, Andrew Troy, Dennis Gyomber , David Webb, Damien Bolton, Nathan Lawrentschuk Department of Urology, Austin Health, Melbourne, Victoria, Australia. Posters Proudly Supported by: . Introduction

E N D
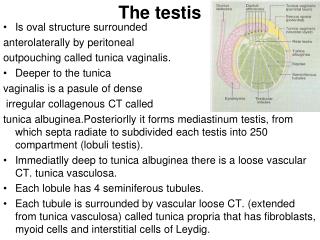
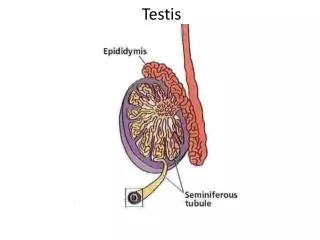
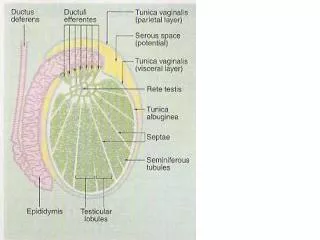
No. 032 Vasculitic Infarction of the testis – Is organ sparing possible? David Pan, Andrew Troy, Dennis Gyomber, David Webb, Damien Bolton, Nathan Lawrentschuk Department of Urology, Austin Health, Melbourne, Victoria, Australia Posters Proudly Supported by: Introduction Testicular infarction as a result of systemic vasculitis is an exceptionally rare entity. Young patient commonly presents with painful scrotum without other urinary symptoms or signs. Differentiating vasculitic infarction from testicular tumour can be challenging. Results A total of 2 patients presented with acute scrotal pain from vasculitic infarction. They had no palpable testicular mass on examination. Both patients had negative tumour markers. Ultrasound of the testes demonstrated ill - defined heterogeneous areas with normal vascularity. They had no symptoms or signs to suggest a systemic vasculitic process. Both patients had exploration of the testis via an inguinal approach. The testis was bivalvedand frozen sections utilised to exclude malignancy. Both patients had testis-sparing surgery. Polyarteritisnodosa(PAN) is a necrotising vasculitis of small and medium sized arteries that may affect any organ. Patients with systemic PAN infrequently present with lethargy, weight loss, hypertension, haematuria and fever of unknown origin(1). Testicular and epididymis are involved in 60-86% of patients with polyarteritisnodosa, however only 2% -18% becomes symptomatic. Vasculitic lesion are commonly hypo-echoic on ultrasound (2), mimicking other benign intra-testicular lesion such as abscess or focal orchitis. Vasculitislesions differ from tumour on US in that they have normal or reduced vascular flow. On T2 weight MRI, low signal peripheral foci abutting the tunica albuginea can be seen (3). Figure 1 Ultrasound Figure 2 T2 weighted MRI Intra-operative ultrasound guided excision biopsy with frozen section is a viable option for suspected vasculitic infarction of the testis(4). With this operative approach, the testis is delivered through inguinal incision. Rubber shod vascular clamp is then placed on the cord and testis placed in cold ischaemia. A 30 French gauge needle is used during US localisation and microsurgical resection carried out. Tissue obtained is sent for frozen section. The accuracy of frozen section is 100% in differentiate benign and malignant lesion and 90% in differentiate between seminoma and Non-seminomatous germ cell tumours (5). Aim To review literature on testicular infarction and describe the imaging and intra-operative techniques to aid organ preservation. Methods The medical records of patients who had inguinal orchidectomy and testicular exploration between 2000 and 2012 were reviewed retrospectively. All patients diagnosed with testicular tumor were excluded from the study. Patients with testicular infarction as a result of vasculitis were noted. Their presentations, pre-operative imaging, intra-operative findings and organ-sparing surgical techniques were discussed. Conclusions Testicular infarction from vasculitis is rare and it is a challenge differentiating it from testicular tumour. With a high index of suspicion, aided by pre-operative ultrasound or MRI, highly selected patients with small lesion may undergo intra-operative exploration and frozen section to achieve organ preservation. • References • 1 Testicular vasculitis: implications for systemic disease. Shurbaji MS, Epstein JI. Hum Pathol 1988; 19:186-9. 1. • 2 Autoimmune testicular vasculitis. Raj GV, Ellington KS, Polascik TJ. Urology2003; 61:1035. • 3 MR imaging of vasculitis of the testis. Hayward I, Trambert MA, Mattrey RF, et al. J Comput Assist Tomogr 1991; 15:502-4.4 • 4 Ultrasound guided needle localization and microsurgical exploration for incidental non palpable testicular tumors. • Hopps CV, Goldstein M, J Urol September 2002 • 5 Accuracy of Frozen Section Examination of testicular tumour of uncertain origin, Elert A, Olbert P, Hegele A, et al. Eur Urol. 2002 Mar;41(3):290-3.