Download
1 / 70
750 likes | 1.02k Views
Neoplasms of the Testis. Ch. 31 Omar Alhunaidi. Introduction. 95% of testicular neoplasms are germ cell tumors ( GCTs ) GCTs are broadly categorized as seminoma and nonseminoma ( NSGCT )

E N D
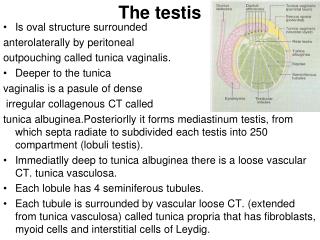
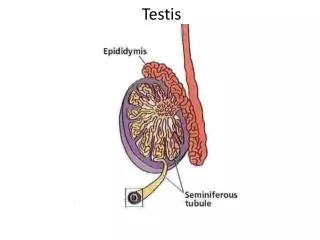
Neoplasms of the Testis Ch. 31 Omar Alhunaidi
Introduction • 95% of testicular neoplasms are germ cell tumors (GCTs) • GCTs are broadly categorized as seminoma and nonseminoma (NSGCT) • GCTs are relatively rare malignancies, accounting for 1% to 2% of cancers among men in the US
Approximately 90% of GCTs arise in the testis and 2% to 5% are extragonadal • long-term survival for men with metastatic GCT is 80% to 90%
Non-GCTs of the testis are rare and include: • sex cord/stromal tumors • lymphoid and hematopoietic tumor • tumors of the collecting duct • tumors of the testicular adnexa
Epidemiology • In the US testicular cancer is the most common malignancy among men aged 20 to 40 years • It is the second most common cancer after leukemia among males aged 15 to 19 years • The incidence of bilateral GCT is approximately 2% • Testicular lymphoma is less common than GCT but it is the most common testicular tumor in men > 50 years
Risk Factors • Four well-established risk factors: • Cryptorchidism ( risk increase 4 to 6 times) • Family history of testicular cancer • Personal history of testicular cancer • Intratubulargerm cell neoplasia (ITGCN) * Infertile men also have a higher incidence of testicular cancer
Most GCTs arise from a precursor lesion called intratubulargerm cell neoplasia (ITGCN) (which is also referred to as carcinoma in situ). • ITGCN is present in adjacent testicular parenchyma in 80% to 90% cases of invasive GCT • Gene expression profile analysis indicates that ITGCN develops before birth from an arrested gonocyte
In men with a history of GCT, the finding of testicular microlithiasis on ultrasound evaluation of the contralateral testis is associated with an increased risk of ITGCN (Karellaset al, 2007). • However, the significance of microlithiasisin the general population is unclear
Pathogenesis and Biology • The carcinogenesis of GCTs is poorly understood • Testicular GCTs develop from a precursor lesion, ITGCN, which, in turn, appears to develop from arrested primordial germ cells or gonocytesthat failed to differentiate into prespermatogonia Hussain et al, 2008 • Approximately 70% of GCTs have an extra copy of chromosome 12 in the form of an isochromosome 12p (i[12p]
Increased incidence of other male reproductive disorders, such as: • Hypospadias • Cryptorchidism • Subfertility • These findings led to the hypothesisthat testicular cancer and these other disorders all resulted from a TESTICULAR DYSGENESIS SYNDROME, which is due to environmental and/or lifestyle factors
Environmental and/or lifestyle factors: • Increased prenatal estrogen exposure • reduction in androgen activity • mothers of children with testicular cancer have more pollutant in their blood • *ALL ARE HYPOTHESIS
GCTs is sensitive to cisplatin-based chemotherapy, which enables cure in the vast majority of patients with widely metastatic disease.
Up to 10% of GCTs are extragonadal • 2 main hypothesis: • they originate from germ cells that mismigratedalong the genital ridge and were able to survive in an extragonadalenvironment • Reverse migration from the testis to extragonadallocations
Histologic Classification • GCTs classified as: • Seminoma (52% to 56%) • NSGCT (44% to 48%) • Embryonalcarcinoma(EC) • yolksac tumor • Teratoma • choriocarcinoma
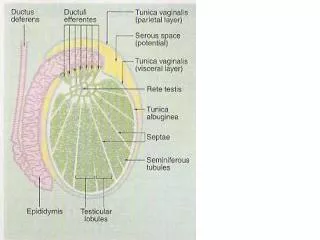
Intratubular Germ Cell Neoplasia • all adult invasive GCTs arise from ITGCN except for spermatocytic seminoma • consists of undifferentiated germ cells that have the appearance of seminoma that are located basally within the seminiferous tubules • tubule usually shows decreased or absent spermatogenesis • presence of ITGCN in an orchiectomy specimen in men with testicular cancer does not carry any prognostic implications
Seminoma • Seminoma is the most common type of GCT • Most cases diagnosed in the fourth or fifth decade • Grossly, seminoma is a soft tan to white diffuse or multinodular mass
SpermatocyticSeminoma • Rare and accounts for less than 1% of GCTs • Unlike other GCTs: • does not arise from ITGCN • not associated with a history of cryptorchidism • does not express PLAP or i(12p) • does not occur as part of mixedGCTs • It is a benign tumor (only one documented case having metastasized) and is almost always cured with orchiectomy (Chung et al, 2004a).
EmbryonalCarcinoma. • most undifferentiated cell type of NSGCT, with totipotentialcapacity to differentiate to other NSGCT cell types • Grossly, it is a tan to yellow neoplasm that often exhibits large areas of hemorrhage and necrosis • aggressive tumor associated with a high rate of metastasis, often in the context of normal serum tumor markers
Choriocarcinoma • rare and aggressive tumor • typically presents as elevated serum hCG levels and disseminated disease • commonly spreads by hematogenousroutes • common sites of metastases: • Lungs • Brain ( DON’T FRGET TO IMAGE THE BRAIN) • Eyeand skinmetastases are also been reported
Yolk Sac Tumors • Pure yolk sac tumors represent a very small fraction of adult-type GCTs but are more common in mediastinal and pediatric GCTs • Schiller-Duvalbody is a characteristicfeature • almost always produce AFP but not hCG
Teratomas • are tumors that contain well-differentiated orincompletely differentiated elements of at least two of the threegerm cell layers of: • endoderm • mesoderm • Ectoderm • Teratomas are generally associated with normal serum tumor markers, but they may cause mildly elevated serum AFP levels • In adults, teratomas are histologically benign but are frequently found at metastatic sites in patients with advanced NSGCT • Teratoma is resistant to chemotherapy
Growing TeratomaSyndrome: • Is when teratoma grows uncontrollably, invade surrounding structures, and become unresectable • Rarely, it may transform into a somatic malignancy such as rhabdomyosarcoma, adenocarcinoma, or primitive neuroectodermal tumor • Malignanttransformation is highly aggressive, resistant to conventional chemotherapy, and associated with a poor prognosis
Initial Presentation • The most common presentation of testicular cancer is a painless testicular mass • Acute testicular pain is less common and is caused by rapid expansion of the testis due to intratumor hemorrhage or infarction • Pain is more commonly associated with NSGCT, because these tumors tend to be more vascular and exhibit more rapid growth • Symptoms related to metastatic disease are the presenting complaint in 10% to 20% of patients
Retroperitoneal metastasis may cause: • palpable mass • abdominal pain • flank pain due to ureteral obstruction • back pain due to involvement of the psoas muscle or nerve roots • lower extremity swelling due to compression of the inferior vena cava • gastrointestinalsymptoms.
Pulmonary metastasis may present as • dyspnea • chest pain • cough • hemoptysis • Metastasis to supraclavicular lymph nodes may present as • neck mass
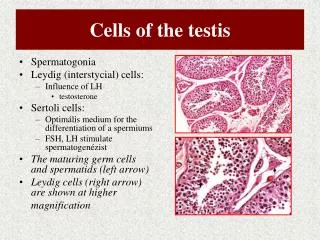
Approximately 2% of men have GYNECOMASTIA, resulting from either: • elevated serum hCGlevels • decreased androgen production • increased estrogen levels (most commonly seen in men withLeydigcelltumors) • Although approximately two thirds of men with GCT have diminished fertility, it is an uncommon initial presentation
Physical Examination • physician should carefully examine both testis • Atrophy of the affected or contralateral testis is common, more with h/o cryptorchidism • Any firm area within the testis is suggestive of malignancy • hydrocele may accompany a testicular cancer and impair the examination
Patient should also be examined for any evidence of: • palpable abdominal mass or tenderness • inguinal lymphadenopathy (mainly if he had prior inguinal or scrotal surgery) • gynecomastia • supraclavicular lymphadenopathy • Auscultation of the chest
A firm intratesticularmass should be considered cancer until proven otherwise and should be evaluated further with scrotal U/S
Diagnostic Testing • Scrotal U/Sshould be considered after examination because it is inexpensive and noninvasive • On ultrasonography the typical GCT is hypoechoicand two or more discrete lesions may be identified • Heterogeneousechotexturewithin a lesion is more commonly associated with NSGCT, because seminomas usually have a homogeneous echotexture
Serum Tumor Markers • LDH • AFP • hCG • They are essential in its diagnosis, prognosis, treatment, and monitoring • AFP is elevated in: • 50% to 70% of low-stage(CS I, IIA, IIB) NSGCT • 60% to 80% of advanced(CS IIC, III) NSGCT
EC andyolk sac tumorssecrete AFP • Choriocarcinomasand seminomas do not produce AFP • The half-life of AFP is 5 to 7 days • AFP levels may also be raised in patients with • hepatocellular carcinoma • Stomach ca • Pancreas ca • biliary tract ca • Lungca
hCG levels are elevated in • 20% to 40% of low-stage NSGCT • 40% to 60% of advanced NSGCT • 15% of seminomas secrete hCG • hCG is also secreted by choriocarcinoma and EC • The half life of hCG is 24 to 36 hours
hCG levels may be elevated in cancers of the: • liver • biliary tract • pancreas • stomach • lung • Breast • kidney • bladder
LDH levels are elevated in: • 20% of lowstageGCTs • 20% to 60% of advanced GCTs • LDH is expressed in smooth, cardiac, and skeletal muscle • Lymphomamay also cause elevated LDH levels
Patients suspected of having a GCT should do serum AFP, hCG, and LDH evaluation • beforeorchiectomyto aid in the diagnosis • and to help interpret postorchiectomytumor marker levels
Initial Management • Radical inguinal orchiectomy when testicular neoplasm is suspected, with removal of the tumor-bearing testis and spermatic cord to the level of the internal inguinal ring • A transscrotal orchiectomy or biopsy is contraindicated because: • it leaves the inguinal portion of the spermatic cord intact and may alter the lymphatic drainage of the testis • increasing the risk of local recurrence • Pelvic oringuinal lymph node metastasis
Because of the rapid growth of GCT, orchiectomy should performed in a timely manner and delays greater than 1 to 2 weeks should be avoided
Testis-sparing surgery (or partial orchiectomy) • is highly controversial and has no role in the patient suspected of having a testicular neoplasm with a normal contralateral testis • It MAYbe considered for organ confined tumors of less than 2 cm in patients with bilateral tumors or tumor in a solitary testis • Also it may be considered for suspected benign tumor or indeterminate lesion when serum AFP, hCG, and LDH values are normal.
When testis-sparing surgery is performed,biopsies of the adjacent testicular parenchyma should be done to R/O ITGCN • Adjuvant radiotherapy to the residual testis is usually sufficient to prevent the development of a GCT
Biopsy of the Contralateral Testis • Open inguinal biopsy of the contralateral testis may be considered in patients with risk factors for ITGCN or those with suspicious lesions on preoperative ultrasonography
Clinical Staging • The prognosis of GCT and initial management decisions are dictated by the clinical stage of the disease by histological and radilogical findings • Lymphatic spread is the most common route of disease dissemination, except for Choriocarcinoma. • Retroperitoneumis the initial site of metastatic spread in 70% to 80% of patients with GCT
Clinical Staging • CS I : disease clinically confined to the testis • CS II : indicates the presence of regional (retroperitoneal) lymph node metastasis • CS III : represents nonregional lymph node and/or visceral metastasis.
For RIGHT testicular tumors the primary drainage site is the interaortocaval lymph nodes inferior to the renal vessels, followed by the paracaval and para-aortic nodes. • For LEFTtesticulartumors is the para-aortic lymph nodes, followed by the interaortocaval nodes • Distal iliac and inguinal lymph nodes secondary to large volume diseaseor aberrant testicular lymphatic drainage
All patients with GCT should do CT Abd+Pelvis with oral & IV contrast for staging • (MRI) is an alternative to CT
ChestImaging • All patients with GCT should undergo chest imaging • Thoracic metastasis in the absence of retroperitoneal disease and/or elevated serum tumor markers is uncommon • Routinechest CT may be associated with a high rate of false-positive findings
Serum Tumor Markers • Postorchiectomy AFP, hCG, and LDH levels are important for staging, prognosis, and treatment selection • presence of newly elevated and/ or rising serum tumor marker levels after orchiectomy indicates metastatic disease