Download

1 / 35
370 likes | 1.05k Views
Mastitis. SURENDRA SINGH, 318. Mastitis. An acute inflammation of the interlobular connective tissue within the mammary gland. Mastitis. Normal breast architecture. Outline. Epidemiology Presentation Predisposing factors Microbiology Treatment Complications Effect on breast milk.

E N D
Mastitis SURENDRA SINGH, 318
Mastitis An acute inflammation of the interlobular connective tissue within the mammary gland
Mastitis Normal breast architecture
Outline • Epidemiology • Presentation • Predisposing factors • Microbiology • Treatment • Complications • Effect on breast milk
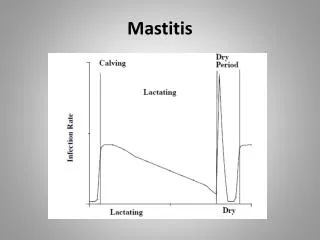
Epidemiology • Incidence 2-33% • ACOG reports 1-2% in U.S. • Most common worldwide <10% • Most common 2nd-3rd week postpartum • 74-95% in first 12 weeks • Can occur anytime in lactation
Presentation • Systemic illness: Chills, myalgias • Fever of ≥ 38.5 • Tender, hot, swollen wedge-shaped erythematous area of breast • Usually one breast
Differential Diagnosis • Fullness: bilateral, hot, heavy, hard, no redness • Engorgement: bilateral, tender, +/- fever, minimal diffuse erythema • Blocked Duct: painful lump with overlying erythema, no fever, feel well, particulate matter in milk
Differential Diagnosis • Galactocele: smooth rounded swelling (cyst) • Abscess: tender hard breast mass, +/- fluctuance, skin erythema, induration, +/- fever • Inflammatory Breast Carcinoma: unilateral, diffuse and recurrent, erythema, induration
Causes • Milk Stasis • Stagnant milk increases pressure in breast leading to leakage in surrounding breast tissue • Milk, itself, causes an inflammatory response • +/- Infection • Milk provides medium for bacterial growth
Causes • 3 groups • Milk stasis (bacteria<10^3, leuk<10^6) • Noninfectious inflammation (bacteria <10^3, leuk >10^6) • Infectious (bacteria >10^3, leuk>10^6) • Randomized treatment • No intervention • Systematic emptying of breast • Infectious group with 3rd intervention: antibiotics (PCN, Amp, Erythro) and systematic emptying
Causes • “Poor results” • Milk stasis (10) – 3 recurrences, 7 impaired lactation • Noninfectious (20) – 13 recurrences • Infectious (76 – only 2 in Abx group) – 6 abscesses, 21 recurrences • Could not clinically tell difference between the groups without lab data. • Conclusion: Treat with antibiotics
Predisposing factors • Improper nursing technique • Timing of feeds • Poor attachment • Oversupply of milk • Overabundant milk supply • Lactating for multiples • Rapid weaning • Blocked nipple pore or duct • Pressure on Breast • Tight Bra • Car seatbelt (yes, this is actually listed) • Prone sleeping position
Predisposing factors • Damaged nipple (nipple fissure) • Primiparity • Previous history of mastitis • Maternal or neonatal illness • Maternal stress • Work outside the home • Trauma • Genetic
Microbiology • Detection of pathogens difficult • Usually nasal/skin flora • Difficult to avoid contamination • Milk culture • Encouraged in hospital acquired, recurrent mastitis, or no response in 2 days
Microbiology • Staph Aureus • Coag neg staph • Also, Group A and B βhemolytic Strep, E Coli, H. flu • MRSA • Fungal infections • TB where endemic – 1% of cases
Fungal infections • Based on case reports that anti-fungal cream improves sx • Case reports of cyptococcal infection • Most common: Candida Albicans • Genital tract Newborn oral colonization • May lead to nipple fissure • Thought to be associated with deep, shooting pains and nipple discomfort • Most commonly treated with fluconozole to ♀, oral nystatin to infant
Treatment • Supportive Therapy • Rest, fluids, pain medication, anti-inflammatory agents, encouragement • Continue breast feeding • Antibiotics that cover Staph and Strep • Culture results • Severe symptoms • Nipple fissure • No improved after 12-24 hours of milk removal
Treatment(ACOG) • Dicloxicillin 500 mg qid • Erythromycin if PCN allergic • If resistant to treatment penicillinase-producing staph, then vancomycin or cefotetan until 2 days after infection subsides • Minimum treatment 10-14 days
Treatment(Alternative) • Therapeutic U/S • Accupunture • Bella donna, Phytolacca, Chamomilla, sulphur, Bellis perenis • Cabbage leaves • Avoid drinks like coffee with methylxanthines, decreasing fat intake
Complications (Other bad things related to mastitis)
Breast Abscess Breast abscess with early skin necrosis
Abscess • Most common in first 6 weeks • 5-11% of mastitis cases • Affect future lactation in 10% of affected ♀ • No differences b/t groups by age, parity, localization of infection, cracked nipples, + milk cultures, mean lactation time • Duration of symptoms: only independent variable favoring abscess development
Breast Abscess Inflammatory breast cancer
Other Complications • Distortion of breast • Chronic inflammatio
Granulomatous Mastitis • Noncaseating granulomas in a lobular distribution • Differential Diagnosis • TB mastitis • Foreign body • Fat necrosis • Autoimmune: sarcoid, erythema nodusum, polyarthritis • Presentation • Unilateral Breast lump • No infection identified at presentation
Granulomatous Mastitis • Can mimic Breast Ca on clinical, radiological, and cytological exams • Diagnosis: Histology • Treatment: • Antibiotics not helpful • Corticosteroids • Excision biopsy • Limited literature, but no clear association with breast feeding, OCPs
Neonatal Mastitis • Occurs up to 5 weeks of age • Girls outnumber boys 2 : 1 • Etiology: 85% S. aureus, also E. coli, group D Streptococcus • Treatment: • Prompt antibiotics (IV?) • Careful needle aspiration if abscess
Immune Factors • IgA is predominant in milk • Increased immune factors from both plasma and local epithelial cells • No adverse events documented in peds • Poor growth documented likely related to poor milk production • Contradictory studies showing benefit or harm • Interest in pediatric vaccine development Michie 2003, Filteau 2003
Increased HIV transmission risk • Alternating breast/bottle increased risk • Role of free virus vs cell bound virus unclear • If ♀ must breast feed, then pump on affected breast (pasteurize) and feed on unaffected Michie 2003, Filteau 2003