Download
1 / 24
290 likes | 581 Views
Deep Vein Thrombosis. Common, Preventable, and potentially Fatal. Disclaimer. Who am I. W. Robert Leeper, MD PGY IV – General Surgery and Intensive Care Medicine Schulich School of Medicine and Dentistry University of Western Ontario. Why am I giving this talk?.

E N D
Deep Vein Thrombosis Common, Preventable, and potentially Fatal
Disclaimer • Who am I W. Robert Leeper, MD PGY IV – General Surgery and Intensive Care Medicine Schulich School of Medicine and Dentistry University of Western Ontario • Why am I giving this talk? 1) My research is in DVT and PE prevention 2) It’s the last talk of the day and they heard I was ‘energetic’ 3) I’m a resident so I’m very, very cheap
Overview • What IS a DVT/PE and WHY do I care? • When should I SUSPECTa DVT/PE? • How do I DIAGNOSEa DVT/PE? • How do I PREVENT a DVT/PE? • How do I TREAT a DVT/PE?
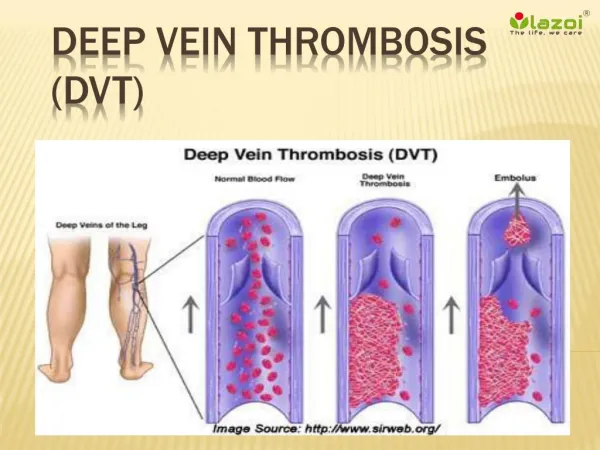
What is a DVT/PE and why do I care? • Definition: • A blood clot forming in a “deep” vein • Usually lower extremity • Etiology = Virchow’s Triad: • Circulatory Stasis • Intimal Injury • Hypercoagulability
What is a DVT/PE and why do I care? • Pulmonary Embolism: • A blood clot that formed in a “deep” vein and then “embolized” back to the heart/lungs • Commonly cited cause of the “late” trauma death
When should I SUSPECT a DVT/PE? First and foremost…….. BE VERY, VERY SUSPICIOUS!!!!
When should I SUSPECT a DVT/PE? LHSC Data (2002 – 2007) • Incidence • < 5% overall • High Risk Injuries • Head Injury (44%) • Lower Limb # (52%) • Pelvic # (37%) • Spinal Cord Injury (15%) • High Risk Event • Major OR < 4h (67%) • SCD Contraindicated (74%) • Prolonged Immobilization (93%) • Missed doses of LMWH (100%) Humphrey, Parry, Girotti, Gray. Unpublished Data – Presented at TAC 2007
When should I SUSPECT a DVT/PE? EAST Practice Guidelines • Incidence • 5 – 10 % overall • High Risk Injuries • Spinal Cord Injury (LEVEL I) • Lower Limb # (LEVEL II) • Pelvic # (LEVEL II) • Head Injury (LEVEL II) • High Risk Factors • Older age (LEVEL II) • Higher ISS (LEVEL II) • Blood Transfusions (LEVEL II) Rogers et al. Management of Venous Thromboembolism in Trauma Patients. J Trauma. 53(1):142-164, July 2002.
How do I DIAGNOSE a DVT/PE? • Clinical • Swollen, Painful, Erythematous Extremity • SOB, pleuritic pain, tachypneia, hypoxia • SUDDEN COLLAPSE • Laboratory • D-Dimer • Blood gas, EKG, CXR • Definitive • US leg veins (9 to 5 test) • VQ Scan or CT PE study (24/7 test)
How do I DIAGNOSE a DVT/PE? LHSC Practice • Doppler US in ALL symptomatic patients • Screening US in HIGH RISK patients EAST Practice Guidelines • Doppler US in ALL symptomatic patients (LEVEL I) • Screening US in HIGH RISK patients (LEVEL III)
How do I PREVENT a DVT/PE? • Prevention Strategies • Early Ambulation • Prophylactic Anticoagulation • Mechanical Compression Devices • IVC Filters
How do I PREVENT a DVT/PE? • Early Ambulation • No debate on this topic • Level I evidence • Multiple benefits beyond DVT/PE prevention • Easier said than done ?
How do I PREVENT a DVT/PE? • Prophylactic Anticoagulation • Typically LMWH • Dalteparin 5000 units sc daily • LHSC Practice • LMWH for ALL eligible patients • LMWH given throughout hospital stay
How do I PREVENT a DVT/PE? • Prophylactic Anticoagulation EAST Guidelines • LMWH for specific patients (LEVEL II) (lower extremity #, pelvic #, SCI…) • LMWH for ISS > 9 (LEVEL III) • LMWH specifically contraindicated with intracranial bleeding or epidural catheter (LEVEL III)
How do I PREVENT a DVT/PE? • Mechanical Compression Devices (MCD) • Preferred method if LMWH is contraindicated LHSC Practice • MCD for ALL eligible patients EAST Guidelines • MCD may not reduce rates of DVT/PE (LEVEL II) • MCD may be indicated for SCI patients (LEVEL III)
How do I PREVENT a DVT/PE? • IVC Filters • What are they? • How do they work? • When should we use them?
How do I PREVENT/TREATa DVT/PE? • IVC Filters • Traditional Indications (LEVEL 1) • Known DVT + contraindication to anticoagulation • Recurrent PE while on anticoagulation • “Extended” Indications (LEVEL II) • Free floating clot in iliac/IVC • Following ‘massive’ PE • “Prophylactic” Indications (LEVEL III) • Any high risk injury type + contraindication to anticoagulation (SCI, Pelvic #, Extremity #, Severe closed head…)
How do I PREVENT/TREAT a DVT/PE? • IVC Filters – LHSC Experience • 2000 – 2008 • n = 27 filters • Very selective utilization • 85% retrieval rate • Impressive retrieval rate Leeper, Gray, Kribs, Parry. Unpublished Data – Presented at ATS/TAC 2009
How do I PREVENT/TREAT a DVT/PE? • IVC Filters – LHSC Experience VTE Prophylaxis 3 (11%) Indication for Placement of IVCF in Trauma Patients 14 (52%) 10 (37%) DVT PE (contraindication for anticoagulation) (contraindication for anticoagulation) N = 27 Leeper, Gray, Kribs, Parry. Unpublished Data – Presented at ATS/TAC 2009
How do I PREVENT/TREAT a DVT/PE? • IVC Filters – LHSC Experience Irretrievable due to trapped clot 2 (7%) Died of Injuries 2 (7%) Figure 2 – Indication for Retrieval/Non Retrieval of IVCF 23 (85%) Successfully retrieved N = 27 Loss to Follow Up Rate = 0% Leeper, Gray, Kribs, Parry. Unpublished Data – Presented at ATS/TAC 2009
How do I PREVENT/TREAT a DVT/PE? • Treatment of Known DVT/PE • Full Dose Anticoagulation • IV Heparin infusion • Fragmin at HIGH dose (200 u/kg) • IVC Filter • If anticoagulation contraindicated • Thrombolyticsvs Surgical Embolectomy • Indicated for MASSIVE pulmonary embolism
Summary – DVT/PE DVT and PE in Trauma Patients • Maintain a HIGH INDEX of suspicion • Maintain a LOW THRESHOLD to investigate • Prevention >>> Cure
Thank you Dr. W. Robert Leeper MD General Surgery and Critical Care Medicine - PGY IV Schulich School of Medicine and Dentistry The University of Western Ontario Rob.Leeper@gmail.com