Download
1 / 43
770 likes | 3.15k Views
Deep Vein Thrombosis. Jane Chun-wen Teng D.O. 11/14/12. Overview of the Causes for Deep Vein Thrombosis. The most common presentations of venous thrombosis are deep vein thrombosis (DVT) of the lower extremity and pulmonary embolism.

E N D
Deep Vein Thrombosis Jane Chun-wen Teng D.O. 11/14/12
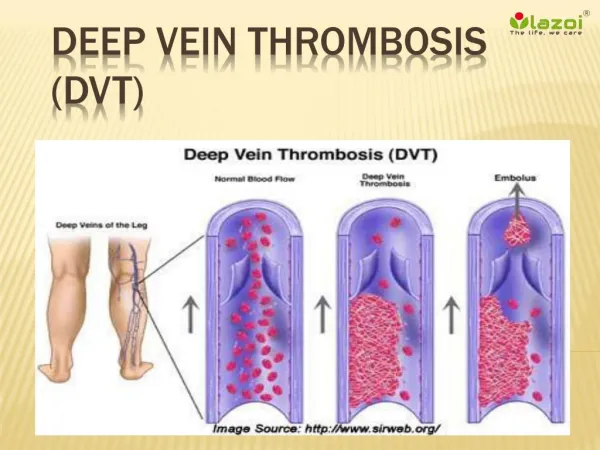
Overview of the Causes for Deep Vein Thrombosis • The most common presentations of venous thrombosis are deep vein thrombosis (DVT) of the lower extremity and pulmonary embolism. • Distal (calf) vein thrombosis, in which thrombi remain confined to the deep calf veins • Proximal vein thrombosis, in which thrombosis involves the popliteal, femoral, or iliac veins • Proximal vein thrombosis is of greater importance clinically, since it is more commonly associated with the development of pulmonary emboli. • The causes of venous thrombosis can be divided into two groups: hereditary and acquired.
Virchow’s Triad • VIRCHOW'S TRIAD — A major theory delineating the pathogenesis of venous thromboembolism (VTE), often called Virchow's triad • Alterations in blood flow (ie, stasis) • Vascular endothelial injury • Alterations in the constituents of the blood (ie, inherited or acquired hypercoagulable state)
Epidemiology Among 1102 acutely ill, immobilized general medical patients enrolled in the MEDENOX study, multiple logistic regression analysis found the following factors to be significantly and independently associated with an increased risk for VTE, most of which were asymptomatic and diagnosed by venography of both lower extremities • Presence of an acute infectious disease • Age >75 years • Cancer • History of prior VTE
Risk Factors for DVT • History of immobilization or prolonged hospitalization/bed rest • Recent surgery • Obesity • Prior episode(s) of venous thromboembolism • Lower extremity trauma • Malignancy • Use of oral contraceptives or hormone replacement therapy • Pregnancy or postpartum status • Stroke
History of DVT • History — Classic symptoms of DVT include swelling, pain, and erythema of the involved extremity. There is not necessarily a correlation between the location of symptoms and the site of thrombosis. Symptoms in the calf alone are often the presenting manifestation of significant proximal vein involvement, while some patients with whole leg symptoms are found to have isolated calf vein DVT. • A complete thrombosis history includes the age of onset, location of prior thromboses, and results of objective diagnostic studies documenting thrombotic episodes in the patient.
History of DVT • The patient should be carefully questioned concerning recent potential precipitating conditions prior to the time of thrombosis, such as surgical procedures, hospitalization, trauma, pregnancy, heart failure, and immobility. • Women should be carefully questioned regarding use of oral contraceptives or hormone replacement therapy as well as their obstetric history. The presence of recurrent fetal loss in the second or third trimester suggests the possible presence of an inherited thrombophilia or antiphospholipid antibodies. • In addition to events proximate to the time of thrombosis, patients should also be questioned about previous exposure and outcome in situations that predispose to thrombosis, such as pregnancy, cesarean section, and surgery.
History of DVT • Questions should include the presence of significant disorders, such as collagen-vascular disease, myeloproliferative disease, atherosclerotic disease, or nephrotic syndrome and about the use of drugs which can induce antiphospholipidantibodies such as hydralazine, procainamide, and phenothiazine. • The patient should also be questioned about a past history of cancer, and the results, if any, of regular screening examinations for cancer since recurrent thrombosis in spite of therapeutic anticoagulation with oral anticoagulants is more frequent in patients with VTE in association with active cancer or an occult neoplasm. • Other findings that may suggest an underlying malignancy are constitutional symptoms such as loss of appetite, weight loss, fatigue, pain, hematochezia, hemoptysis, and hematuria
Family History of DVT • A positive family history of VTE is particularly important, since a well documented history of VTE in one or more first-degree relatives under age 50 suggests the presence of a hereditary defect and/or an increased susceptibility for venous thromboembolic disease. • This was most conclusively shown in a population-based study of the incidence of VTE according to the presence or absence of VTE in a sibling. • Standard incidence ratios for VTE were 2.27, 51.9, and 53.7 for patients with one, two, or three or more affected siblings, respectively.
Special Clinical Settings • There a number of clinical settings which may suggest the presence of a specific risk factor for DVT. As examples: • Recurrent unprovoked DVT in a young patient (age <50) may suggest either the presence of an inherited hypercoagulable state or a congenital anomaly of the inferior vena cava. • Recurrent left lower extremity DVT of the left lower extremity may indicate the presence of the May-Thurner syndrome with thrombosis of the left iliac vein due to compression of this vein between the overlying right iliac artery and the vertebral column.
Physical Exam • Physical examination may reveal a palpable cord (reflecting a thrombosed vein), calf or thigh pain, unilateral edema or swelling with a difference in calf diameters, warmth, tenderness, erythema, and/or superficial venous dilation. • In the general physical examination, special attention should be directed to the vascular system, extremities (eg, looking for signs of superficial or deep vein thrombosis), chest, heart, abdominal organs, and skin (eg, skin necrosis, livedoreticularis).
Physical Exam • There may be pain and tenderness in the thigh along the course of the major veins. Tenderness on deep palpation of the calf muscles is suggestive, but not diagnostic. Homans’ sign is also unreliable. • However, each of the above signs and symptoms is nonspecific and has low accuracy for making the diagnosis of DVT. A 2005 meta-analysis of diagnostic cohort studies of patients with suspected DVT concluded the following concerning these physical findings
Physical Exam • Only a difference in calf diameters (likelihood ratio, LR 1.8; 95% CI 1.5-2.2) was of potential value for ruling in DVT. • Only absence of calf swelling (LR 0.67; 95% CI 0.58-0.78) and absence of a difference in calf diameters (LR 0.57; 95% CI 0.44-0.72) were of potential value for ruling out DVT. • Individual clinical features are poorly predictive of DVT when not combined in a formal prediction rule (e.g. Wells score) • Accordingly, further diagnostic testing is required to confirm or exclude the diagnosis of DVT
Physical Exam • Venous thromboembolism may also be associated with other clinical disorders such as heart failure and the myeloproliferative neoplasms. The presence or absence of relevant physical exam findings (e.g., splenomegaly in polycythemia vera) should be ascertained. • The physical examination may also reveal signs of hepatic vein thrombosis (Budd-Chiari syndrome), such as ascites and hepatomegaly, or edema due to the nephrotic syndrome. The hypercoagulable state associated with the nephrotic syndrome may manifest as renal vein thrombosis, which is usually asymptomatic unless associated with pulmonary embolism.
Physical Exam • Phlegmasiaceruleadolens — Phlegmasiaceruleadolens is an uncommon form of massive proximal (eg, iliofemoral) venous thrombosis of the lower extremities associated with a high degree of morbidity and mortality. • Signs and symptoms include sudden severe leg pain with swelling, cyanosis, edema, venous gangrene, compartment syndrome, and arterial compromise, often followed by followed by circulatory collapse and shock. Delay in treatment may result in death or loss of the patient's limb.
Physical Exam • Screening for malignancy — Since venous thromboembolism may be the first manifestation of an underlying malignancy, rectal examination and stool testing for occult blood should be performed and women should undergo a pelvic examination to rule out the presence of a previously unsuspected pelvic mass or malignancy. However, a routine exhaustive search for an occult malignancy is neither warranted nor cost effective.
Laboratory Testing • The initial laboratory evaluation in patients with venous thrombosis should include a complete blood count and platelet count, coagulation studies (eg, prothrombin time, activated partial thromboplastin time), renal function tests, and urinalysis. • Consideration should be given to obtaining a prostate-specific antigen measurement in men over the age of 50. Any abnormality observed on initial testing should be investigated aggressively.
Differential Diagnosis • When approaching the patient with suspected DVT of the lower extremity, it is important to appreciate that only a minority of patients (17 and 32 percent in two large series) actually have the disease • Muscle strain, tear, or twisting injury to the leg — 40 percent • Leg swelling in a paralyzed limb — 9 percent • Lymphangitis or lymph obstruction — 7 percent • Venous insufficiency — 7 percent • Popliteal (Baker's) cyst — 5 percent • Cellulitis — 3 percent • Knee abnormality — 2 percent • Unknown — 26 percent
Diagnosis of DVT • A number of invasive and non-invasive approaches are possible (eg, contrast venography, impedance plethysmography, compression ultrasonography, D-dimer testing). • In most circumstances, compression ultrasonography is the noninvasive approach of choice for the diagnosis of symptomatic patients with a first episode of suspected DVT • A negative D-dimer assay may be insufficient to rule out DVT as a stand-alone test in patient populations with a high prevalence of venous thromboembolism, and not all D-dimer assays are validated for this application. However, a D-dimer level <500 ng/mL by ELISA or a negative SimpliRED assay in conjunction with a low clinical probability (ie, Wells score)or other negative noninvasive tests may be useful in excluding DVT, without the need for ultrasound testing.
Diagnosis of DVT • A positive noninvasive study in patients with a first episode of DVT usually establishes the diagnosis, with a positive predictive value for compression ultrasonography of 94 percent (95% CI: 87-98 percent). If the initial study is negative and the clinical suspicion of DVT is high, a repeat study should be obtained on day 5 to 7. • Use of a single study via extended (complete) lower extremity ultrasonography may obviate the need for repeat testing. However, this technique requires specialized instrumentation and is highly dependent on user expertise. • Venography is currently used only when noninvasive testing is not clinically feasible or the results are equivocal.
Diagnosis of DVT • Pretest probability — Ultrasonography and D-dimer tests for DVT are most useful when the results are combined with an assessment of pretest probability of DVT. One report of 593 patients with suspected DVT validated a measure of pretest probability (Wells score) • VT was documented in 3, 17, and 75 percent of patients with low, moderate, or high pretest probabilities, respectively.
Well Score • A review of 15 studies in which the Wells score was tested concluded the following • Patients in the low pretest probability category had a median negative predictive value for DVT of 96 percent (range: 87 to 100 percent), indicating the usefulness of the Wells score for ruling out DVT. • The median negative predictive value for DVT in patients with a low pretest probability was improved further by the presence of a negative test for D-dimer (median value 99 percent, range: 96 to 100 percent). • Positive predictive values for DVT rarely exceeded 75 percent for patients in the high pretest probability category, indicating that these rules alone were not as useful for identifying patients who did have thrombosis.
Screening for Hypercoagulable state • Inherited and acquired hypercoagulable states — A biologic risk factor for venous thrombosis can be identified in over 60 percent of Caucasian patients under age 50 with a first idiopathic DVT. In addition, there is often more than one factor at play in a given patient. As an example, 50 percent of thrombotic events in patients with inherited thrombophilia are associated with an accompanying acquired risk factor (eg, surgery, pregnancy, use of oral contraceptives). • Some patients have more than one form of inherited thrombophilia or may have combinations of inherited as well as acquired thrombophilic states and are at even greater risk for thrombosis.
Screening for Hypercoagulable state • A thrombophilic state leading to venous thrombosis can be inherited or acquired: • Congenital/inherited (eg, factor V Leiden, protein C deficiency) • Acquired (eg, following orthopedic surgery, antiphospholipid antibody) • Associated with systemic disease (eg, malignancy) • Who to test — There is currently no consensus regarding who to test for inherited thrombophilia.
Screening for Hypercoagulable state • However, the likelihood of identifying an inherited thrombophilia is increased several-fold by screening only patients with one or more of the following: • Initial thrombosis occurring prior to age 50 without an immediately identified risk factor (ie, idiopathic or unprovoked venous thrombosis) • A family history of venous thromboembolism (ie, first-degree relatives with VTE prior to age 50) • Recurrent venous thrombosis • Thrombosis occurring in unusual vascular beds such as portal, hepatic, mesenteric, or cerebral veins • A history of warfarin-induced skin necrosis, which suggests protein C deficiency.
Value of Screening • Value of screening — Although we can identify patients at increased risk for inherited thrombophilia, there is no clear clinical value to screening for the following reasons: • Even if a hypercoagulable workup uncovers abnormalities predisposing to VTE, the strongest risk factor for VTE recurrence is the prior VTE event itself, particularly if idiopathic. • Patients with idiopathic VTE, whether or not they have an identifiable inherited thrombophilia, are at high risk for recurrence (as high as 7 to 8 percent per year in some studies) after warfarin is discontinued, at least for the first few years after the event. • Thus, the presence or absence of an inherited thrombophilia will usually not change the decision regarding length of warfarin therapy.
Value of Screening • Screening information can be used to identify family members with an inherited thrombophilia, but anticoagulant prophylaxis is rarely recommended in asymptomatic affected family members outside of high risk situations. • Screening test interference — A number of factors can interfere with screening tests for thrombophilia (e.g. Acute thrombosis, heparin, and coumadin therapies). • Therefore, it is generally best not to undertake testing at the time of presentation with VTE.
Treatment for DVT • Rationale — The primary objectives of treatment of DVT are to prevent and/or treat the following complications: • Prevent further clot extension • Prevention of acute pulmonary embolism • Reducing the risk of recurrent thrombosis • Treatment of massive iliofemoral thrombosis with acute lower limb ischemia and/or venous gangrene (ie, phlegmasiaceruleadolens) • Limiting the development of late complications, such as the post-thrombotic syndrome, chronic venous insufficiency, and chronic thromboembolic pulmonary hypertension. • Anticoagulant therapy is indicated for patients with symptomatic proximal DVT, since pulmonary embolism will occur in approximately 50 percent of untreated individuals, most often within days or weeks of the event.
Treatment for DVT • Initial therapy — The following recommendations for the treatment of acute venous thromboembolic disease are in accord with the 2012 ACCP evidence-based clinical practice guidelines for antithrombotic and thrombolytic therapy, as well as recommendations of the British Committee for Standards in Hematology, the joint guidelines of the American College of Physicians and the American Academy of Family Physicians, and the American Heart Association/American College of Cardiology. • Patients with DVT or pulmonary embolism should be treated acutely with LMW heparin, fondaparinux, unfractionated intravenous heparin, or adjusted-dose subcutaneous heparin. • Dosing requirements for LMW heparin are different for each LMW product. Minimal elements for early discharge and/or outpatient therapy with LMW heparin or fondaparinux are shown in the table.
Treatment of DVT • When unfractionated heparin is used, the dose should be sufficient to prolong the activated partial thromboplastin time (aPTT) to 1.5 to 2.5 times the mean of the control value, or the upper limit of the normal aPTT range. A survey of available weight-based nomograms supports the view that they represent a safe and cost-effective strategy for unfractionated heparin dosing in a number of different health care settings. • Treatment with LMW heparin, fondaparinus, or unfractionated heparin should be continued for at least five days and oral anticoagulation should be overlapped with LMW fondaparinux, or unfractionated heparin for at least four to five days.
Treatment of DVT • For most patients, warfarin should be initiated simultaneously with the heparin, at an initial oral dose of approximately 5 mg/day. In elderly patients and in those at high risk of bleeding or who are undernourished, debilitated, or have heart failure or liver disease, the starting dose should be reduced. The heparin product can be discontinued on day five or six if the INR has been therapeutic for two consecutive days. • For patients receiving unfractionated heparin (UFH), ACCP Guidelines suggest that platelet counts be obtained regularly to monitor for the development of thrombocytopenia. The frequency and timing of such counts depends upon the clinical situation.
Treatment of DVT • The heparin product should be stopped if any one of the following occurs: a precipitous or sustained fall in the platelet count, or a platelet count <100,000/microL. • The use of thrombolytic agents, surgical thrombectomy, or percutaneous mechanical thrombectomy in the treatment of venous thromboembolism must be individualized. Patients with hemodynamically unstable PE or massive iliofemoral thrombosis (ie, phlegmasiaceruleadolens), and who are also at low risk to bleed, are the most appropriate candidates for such treatment.
Treatment of DVT – IVC filter • Inferior vena caval filter placement is recommended when there is a contraindication to, or a failure of, anticoagulant therapy in an individual with, or at high risk for, proximal vein thrombosis or PE. • It is also recommended in patients with recurrent thromboembolism despite adequate anticoagulation, for chronic recurrent embolism with pulmonary hypertension, and with the concurrent performance of surgical pulmonary embolectomy or pulmonary thromboendarterectomy.
Treatment of DVT • Oral anticoagulation with warfarin should prolong INR to a target of 2.5 (range:2.0-3.0) If oral anticoagulants are contraindicated or inconvenient, long-term therapy can be undertaken with either dose-adjusted unfractionated heparin, LMWH, or fondaparinux. • Because of ease of use, especially in the outpatient setting, LMW heparin or fondaparinux is preferred to unfractionated heparin. • There is insufficient information at the present time to recommend the use of the newer oral anticoagulants (eg, dabigatran, rivaroxaban, apixaban) for the treatment of DVT.
Duration of treatment • Duration of treatment — The duration of anticoagulation therapy varies with the clinical setting as well as with patient values and preferences. • Patients with a first thromboembolic event in the context of a reversible or time-limited risk factor (eg, trauma, surgery) should be treated for three months. • Patients with a first idiopathic thromboembolic event should be treated for a minimum of three months. Following this, all patients should be evaluated for the risk/benefit ratio of long-term therapy.
Duration of Treatment • Indefinite therapy is preferred in patients with a first unprovoked episode of proximal DVT who have a greater concern about recurrent VTE and a relatively lower concern about the burdens of long-term anticoagulant therapy. • In patients with a first isolated unprovoked or provoked episode of distal DVT, three months of anticoagulant therapy, rather than indefinite therapy, appears to be sufficient. • Most patients with advanced malignancy should be treated indefinitely or until the cancer resolves.
Reference • http://www.uptodate.com/contents/overview-of-the-causes-of-venous-thrombosis?source=search_result&search=deep+vein+thrombosis&selectedTitle=6%7E150 • http://www.uptodate.com/contents/deep-vein-thrombosis-and-pulmonary-embolism-in-pregnancy-epidemiology-pathogenesis-and-diagnosis?source=search_result&search=deep+vein+thrombosis&selectedTitle=5%7E150 • http://www.uptodate.com/contents/diagnosis-of-suspected-deep-vein-thrombosis-of-the-lower-extremity?source=search_result&search=deep+vein+thrombosis&selectedTitle=3%7E150 • http://www.uptodate.com/contents/approach-to-the-diagnosis-and-therapy-of-lower-extremity-deep-vein-thrombosis?source=search_result&search=deep+vein+thrombosis&selectedTitle=1%7E150 • http://www.uptodate.com/contents/deep-vein-thrombosis-and-pulmonary-embolism-in-pregnancy-treatment?source=search_result&search=deep+vein+thrombosis&selectedTitle=7%7E150 • http://www.uptodate.com/contents/fibrinolytic-thrombolytic-therapy-in-acute-pulmonary-embolism-and-lower-extremity-deep-vein-thrombosis?source=search_result&search=deep+vein+thrombosis&selectedTitle=4%7E150