Download
1 / 21
250 likes | 1.01k Views
Deep Vein Thrombosis. Lewis, pp. 882-890 Concept 22.4 pp. 1389-1397. Terminology. Sometimes called thrombophlebitis, phlebothrombosis, venous thrombosis, venous thromboembolism Venous thrombosis refers to clot formation in a vein with inflammation Superficial—in small vein (INT site)

E N D
Deep Vein Thrombosis Lewis, pp. 882-890 Concept 22.4 pp. 1389-1397
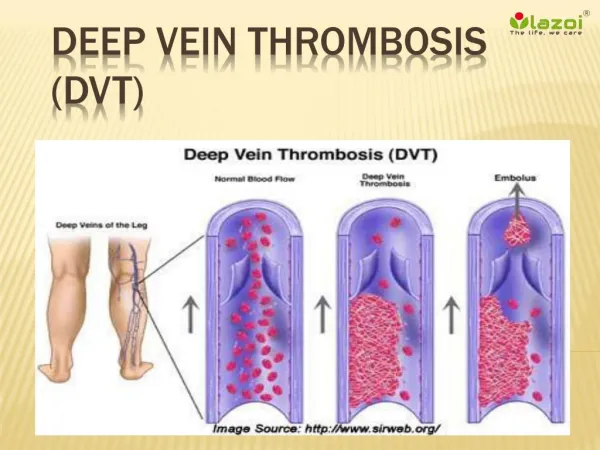
Terminology • Sometimes called thrombophlebitis, phlebothrombosis, venous thrombosis, venous thromboembolism • Venous thrombosis refers to clot formation in a vein with inflammation • Superficial—in small vein (INT site) • Deep—AKA: DVT—located in deep veins, usually iliac or femoral
Etiology • Virchow’s triad: • Venous stasis • Damage of endothelium • Hypercoagulability
Risk Factors for Virchow’s Triad • Venous stasis —incompetent valves, inactivity, obesity, heart failure, afib, orthopedic and pelvic surgeries • Endothelial damage—trauma from various causes, external pressure • Hypercoagulability— blood disorders, sepsis, pregnancy, hormones, smoking
Pathophysiology • When vein is traumatized, inflammation occurs and platelet aggregation and fibrin attract cells to form a thrombus • In venous stasis, clot forms at valve cusps or bifurcations. • If clot gets big enough to occlude vein, manifestations of DVT occur; if not, body will reabsorb it.
Assessment of DVT • 50% are asymptomatic unless the clot is in the ileofemoral vein. • Symptomatic patients and those with ileofemoral clot have edema ,redness, pain, warmth, decreased movement, +Homan’s sign (20% reliable). • Dx Tests: Duplex scanning, venogram, D-dimer blood test
Preventative Management • Antiembolism stockings (TEDs) • Intermittent compression device (DVT boots, Venodynes) • Antiembolism exercises (AEEs) • SQLMWH (Lovenox) • Early ambulation • Encourage fluids • Avoid popliteal pressure, crossing legs
Prevention—Surgical Care Improvement Project • Started in 1999 to identify and implement ways to decrease postoperative complications • Research found that in all major surgical procedures that 25% of pts developed DVT and 7% developed pulmonary embolism • Recommendation was that patients receive prophylaxis within 24h before or after surgery. Could be TEDS, IPCD, LMWH*, ASA.
Core Measures for Venous Thromboembolism (VTE) • VTE Prophylaxis • ICU VTE Prophylaxis • VTE Patients with Anticoagulation Overlap Therapy • VTE Patients Receiving Unfractionated Heparin with Dosages/Platelet Count Monitoring by Protocol • Anticoagulant Discharge Instructions
Elements of Performance: In other words, how does the hospital meet this NPSG? • Reduce the likelihood of patient harm associated with the use of anticoagulant therapy. • Use only oral unit-dose products, prefilled syringes, or premixed infusion bags and make sure they are age-appropriate. • Use only programmable pumps when administering continuous IV heparin • Use approved written protocols for initiation and maintenance of therapy. • Use approved written protocols for addressing baseline and ongoing labs t • Assess baseline coagulation status i.e., INR, PT, PTT. • Manage potential food and drug interactions. • Provide education to prescribers, staff, patients, and families which includes follow-up, compliance, drug-food interactions, adverse reactions • Evaluate these safety practices, make improvements, and measure their effectiveness.
Acute Management • Hospital or home?—depends on size of clot and presence of comorbidities • BR or some degree of ambulation?—EBP has shown no difference • Heat application • Extremity elevation
Acute Pharmacologic Mgmt • IV Heparin—bolus followed by infusion with pump—dosage depends on established hospital protocol • SQ Lovenox q12h—EBP show results as good • PO Warfarin daily—dosage depends on PT, INR • Analgesics—not NSAIDs
Acute Management cont’d • PTT, PT, INR qam—heparin and warfarin doses depend on results; not needed for Lovenox • Monitor for complications—50% develop pulmonary embolism • Surgery—thrombectomy, vena cava filter
Nursing Management of DVT • Practice prevention for at-risk pts. • For acute cases: • Monitor VS, NV status, and extremity measurements • Maintain activity orders • Discourage activities that can cause bleeding • Encourage fluids • Monitor anticoagulants meds and labs • Analgesics and heat • Monitor Vit K in diet • Monitor for complications-PE and hemorrhage
Patient Education • Anticoagulant therapy (890) • Home treatment of DVT (Concept p. 1395) • Prevention • Dietary restrictions related to warfarin tx • Complications • How to give Lovenox at home • Home INR testing • How to apply TEDs
Peripheral Vascular Disease • Affects arteries and veins • Arteriosclerosis--Narrowing and sclerosis of large arteries (femoral, iliac, popliteal) especially at bifurcations due to plaque formation • Chronic Venous Insufficiency—inadequate venous return due to incompetent valves. Venous stasis causes problems with diminished circulation and immune response
Manifestations of PVD • Arterial: • Diminished or absent pulses • Smooth, shiny, dry skin, • No hair • No edema • Round, painful ulcers on distal foot, toes or webs of toes • Dependent rubor • Pallor and pain when legs elevated • Intermittent claudication • Brittle, thick nails • Venous: • Normal pulses • Brown patches of discoloration on lower legs • Dependent edema • Irregularly shaped, usually painless ulcers on lower legs and ankles • Dependent cyanosis and pain • Pain relief when legs elevated • No intermittent claudication • Normal nails • Dermatitis, pruritis
Management of Leg Ulcers • Goals of care: • Promote skin integrity • Increase mobility • Provide good nutrition
Management cont’d • Promoting skin integrity includes good foot care, avoiding trauma, avoiding pressure and standing for long periods. It also includes proper tx of existing ulcers. • Increase mobility as allowed and tolerated. • Good nutrition includes protein, Vits A & C, Fe, Zn, and weight control.
Wound Care Management of Leg Ulcers • Compression tx—stockings, Unna boots, etc. Amount of compression depends on ABI index. • Keep wound moist—irrigate with saline, apply moisture-retentive dressings • Prevent infection using good technique; wound culture if indicated. • For persistent and unresponsive ulcers, surgical debridement, wound vacs, hyperbaric O2 chambers, or skin grafts may be indicated.
Education • Good skin and foot care • Teach pt and family to check feet and skin regularly • Proper diet—Vits A & C, Fe, Zn, weight control • Appropriate activity • Avoidance of trauma • S/S infection • May need to teach patient and family dressing changes