Download
1 / 34
340 likes | 352 Views
Explore the challenges and strategies for achieving 48-hour access to GUM clinics, including shifting activity levels, appointment vs. walk-in services, freeing up capacity, the senior model, home sampling, and results management.

E N D
48-hour access to GUM clinics: is it achievable? 18 may 2019 Dr John White Western & northern Health and Social Care Trusts, N.I.
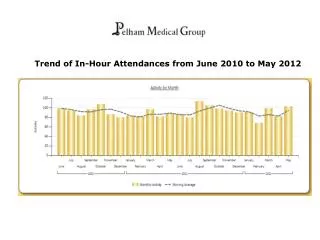
The Reality… • Huge shift in activity from low complexity to higher complexity in target groups (asymptomatic – symptomatic/contacts) • Increase in A/B/C4 diagnoses leads to: • more positive test results to manage • more PN, generating more contacts • more treatments to prescribe/prepare/administer • more pathology (cultures, confirmations) • more recalls for TOCs, RPR follow ups…
Quality standard Published: 5 February 2019 nice.org.uk/guidance/qs178
The Challenge • Do more with less… • Maximise our efficiency • No perfect clinic, no optimal system • Improve flow, reduce waiting times • Focus time/resources on those with most infections/highest risk
High impact changes, 2006 • Undertake service redesign • Improve use of the multidisciplinary team • Separate pathway for screening low risk patients • Improve patient access, clinic opening hours • Maximise the space available for seeing patients • Reduce unnecessary clinical activity
Appointments or walk-in? • Appointment-only services can be troublesome: • High DNA rates often mean wasted capacity and lower activity • Unless appts are prompt, patients with STIs often must wait days-weeks for treatment – risk of complications, onward transmission • BUT – patients like appts and clinicians often prefer the “controlled environment” of an appt clinic
Appointments or walk-in? • Walk-in services more able to fill available capacity with patients • Walk-in every second day (M/W/F) means most clinics could achieve 48-hr access depending on how many they turn away • Not always popular with staff, esp reception • Long waits for patients (2-hr wait in clinic is also a new standard!) • “First-come, first served” doesn’t always allow access for those most at need
Ways to free up capacity • e-Triage, Computer Assisted Self Interview (CASI) • Refine asymptomatic/symptomatic pathways – match patient to clinician competencies • Eradicate slow processes with technology: • E-prescribing/PGDs • E-order comms/sets for pathology tests • Bar-coded stickers for specimens
Ways to free up capacity • E-noting • Is it quicker? • Try to refine multiple proformas for different care scenarios • Limit areas relying on free text • Tick boxes save time! • Don’t include unnecessary info
Senior Model The senior model was introduced when the following changes were embedded: • Patient self-triage • Intensive nurse training • Reception filter based on staff numbers • Matrix to govern patient numbers at the end of the working day
Senior Model A new service model: • one senior clinician asked NOT to directly see patients • instead be on the floor/phone to provide real-time second opinions, advice, prescriptions, teaching, review results etc. across 2 acute sites and 4 community clinics
Reduce unnecessary clinical activity • Stop examining asymptomatic patients! • Stop taking loops from asymptomatic men! • “Slow clinicians”: why are they taking so long? training needs? support? • - work with them to improve efficiency • Routine F/U appts needed? e.g. IUD, PID
Reduce unnecessary clinical activity • “40-80% of medical information provided by healthcare practitioners is forgotten immediately… The greater the amount of information presented, the lower the proportion correctly recalled” • Avoid excessive information giving – use BASHH leaflets and signpost to other sources e.g. SH:24, NHS websites Kessels, RPC. J R Soc Med. 2003
Home sampling • “I want the kit”- established in the US for over a decade (C. Gaydos/Johns Hopkins) • SH:24 – large UK NHS partnership, funded by GSTT charity
Home sampling • SH:24 • Initially for Lambeth & Southwark residents • Home sampling for HIV, syphilis, GC/CT • Now commissioned to deliver free STI testing in 17 other regions in England • regulated by the Care Quality Commission
Results management • All patient should get results • - within 8 working days (BASHH 2019) • Appointments for results kill capacity to see new patients • Phone, SMS, email, automated systems all available…
Results management Int J STD AIDS. 2015 Dec 17 • The provision of HIV results by telephone more than halved the number of men re-attending (74.4% vs. 33.1%) which freed up 516 hours of clinic time
QUDINI queue management • Long waiting times • Frustrated and angry patients… • We introduced new software in October 2014 to see if it could improve patient satisfaction
QUDINI- Patient feedback • Average four complaints a month before we used the queue management software • One complaint re: waiting times in next 2 months • “The texting when you're up was great. Very caring and nice staff.” • “This clinic is very efficient. Love that I received a text stating what my # was in the queue. Thanks for a good experience” • “The text messaging service is a really good idea. Many thanks”
In Summary • More modern & efficient pathways are needed in all clinics • Better demand management = greater capacity – more chance of meeting 48-hour access targets • “Short cuts” don’t necessarily compromise quality of care


![I like [ hour / our ] team the best. hour our](https://cdn1.slideserve.com/2584921/slide1-dt.jpg)